Elizabeth Kachingwe, Nyasha Mutanda, Vinolia Ntjikelane, Mariet Benade, Musa Manganye, Lufuno Malala, Sydney Rosen, Mhairi Maskew
{"title":"特征和六个月病毒载量抑制客户呈现晚期艾滋病病毒病在南非。","authors":"Elizabeth Kachingwe, Nyasha Mutanda, Vinolia Ntjikelane, Mariet Benade, Musa Manganye, Lufuno Malala, Sydney Rosen, Mhairi Maskew","doi":"10.1371/journal.pgph.0004927","DOIUrl":null,"url":null,"abstract":"<p><p>Despite advances in antiretroviral therapy (ART), a notable proportion of individuals still present with advanced HIV disease (AHD) at treatment initiation, defined by CD4 < 200 cells/µL or WHO stage 3/4. This group experiences higher mortality and more opportunistic infections. While guidelines exist, they often do not address AHD clients specific needs early in treatment. Addressing these gaps could improve outcomes. Between September 2022 and June 2023, we surveyed a sequential sample of clients initiating ART or ≤6 months post-initiation at 18 primary healthcare facilities across three provinces. This observational cohort collected socio-demographic data, HIV care history, and service delivery preferences, and linked surveys to routine medical records and described client characteristics using descriptive statistics. Relative risks and risk differences compared outcomes between AHD and non-AHD clients. Primary outcomes were 6-month retention and viral load suppression. Of 1,098 clients (72% female, median age 33), 938 had CD4 or WHO staging at ART start. Of these, 29% (n = 275) had AHD, with a median CD4 of 108 cells/µL. AHD clients were more often male (44% vs. 21%), older (median age: 38 vs. 31 years), and sought care due to illness (63% vs. 33%). TB diagnosis (42% vs. 12%) and testing (76% vs. 67%) were higher. Service preferences and health resource use were similar. Retention at 6 months was similar (80% vs. 75%), but mortality was higher in AHD clients (1.0% vs. 0.2%). AHD clients had more low-level viremia (24% vs. 11%; RR = 2.27, 95% CI = 1.67-3.09) and slightly lower suppression (43% vs. 47%). AHD remains a key barrier to optimal ART outcomes. Clients with AHD experienced poorer viral suppression, despite similar retention rates highlighting the need for early detection, tailored clinical support, and strengthened monitoring. Updating ART guidelines to address AHD-specific needs is critical to improving outcomes in this high-risk population.</p>","PeriodicalId":74466,"journal":{"name":"PLOS global public health","volume":"5 9","pages":"e0004927"},"PeriodicalIF":2.5000,"publicationDate":"2025-09-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12456826/pdf/","citationCount":"0","resultStr":"{\"title\":\"Characteristics and six-month viral load suppression of clients presenting with advanced HIV disease in South Africa.\",\"authors\":\"Elizabeth Kachingwe, Nyasha Mutanda, Vinolia Ntjikelane, Mariet Benade, Musa Manganye, Lufuno Malala, Sydney Rosen, Mhairi Maskew\",\"doi\":\"10.1371/journal.pgph.0004927\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Despite advances in antiretroviral therapy (ART), a notable proportion of individuals still present with advanced HIV disease (AHD) at treatment initiation, defined by CD4 < 200 cells/µL or WHO stage 3/4. This group experiences higher mortality and more opportunistic infections. While guidelines exist, they often do not address AHD clients specific needs early in treatment. Addressing these gaps could improve outcomes. Between September 2022 and June 2023, we surveyed a sequential sample of clients initiating ART or ≤6 months post-initiation at 18 primary healthcare facilities across three provinces. This observational cohort collected socio-demographic data, HIV care history, and service delivery preferences, and linked surveys to routine medical records and described client characteristics using descriptive statistics. Relative risks and risk differences compared outcomes between AHD and non-AHD clients. Primary outcomes were 6-month retention and viral load suppression. Of 1,098 clients (72% female, median age 33), 938 had CD4 or WHO staging at ART start. Of these, 29% (n = 275) had AHD, with a median CD4 of 108 cells/µL. AHD clients were more often male (44% vs. 21%), older (median age: 38 vs. 31 years), and sought care due to illness (63% vs. 33%). TB diagnosis (42% vs. 12%) and testing (76% vs. 67%) were higher. Service preferences and health resource use were similar. Retention at 6 months was similar (80% vs. 75%), but mortality was higher in AHD clients (1.0% vs. 0.2%). AHD clients had more low-level viremia (24% vs. 11%; RR = 2.27, 95% CI = 1.67-3.09) and slightly lower suppression (43% vs. 47%). AHD remains a key barrier to optimal ART outcomes. Clients with AHD experienced poorer viral suppression, despite similar retention rates highlighting the need for early detection, tailored clinical support, and strengthened monitoring. Updating ART guidelines to address AHD-specific needs is critical to improving outcomes in this high-risk population.</p>\",\"PeriodicalId\":74466,\"journal\":{\"name\":\"PLOS global public health\",\"volume\":\"5 9\",\"pages\":\"e0004927\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-09-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12456826/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"PLOS global public health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1371/journal.pgph.0004927\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLOS global public health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pgph.0004927","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Characteristics and six-month viral load suppression of clients presenting with advanced HIV disease in South Africa.
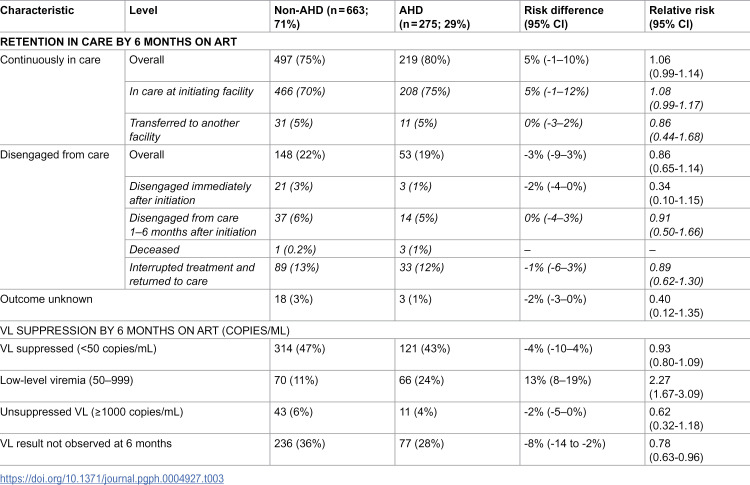
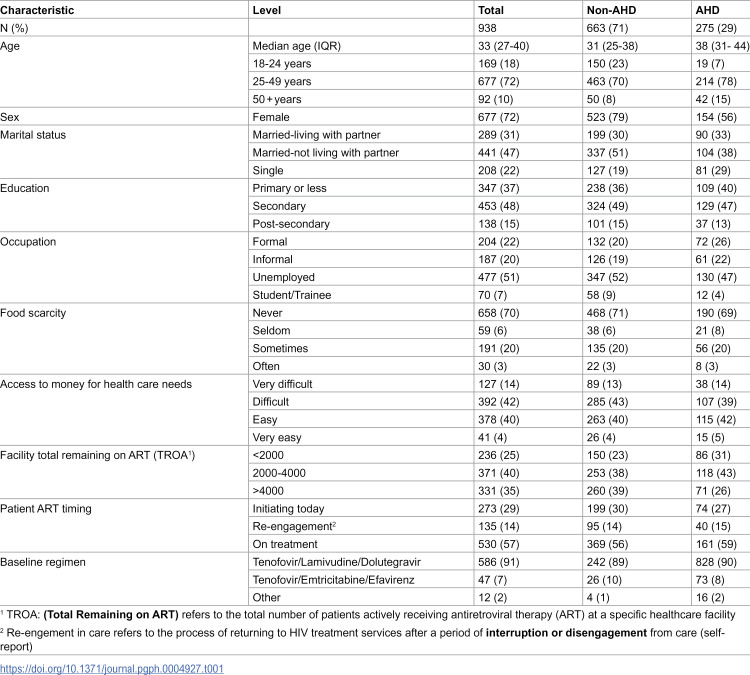
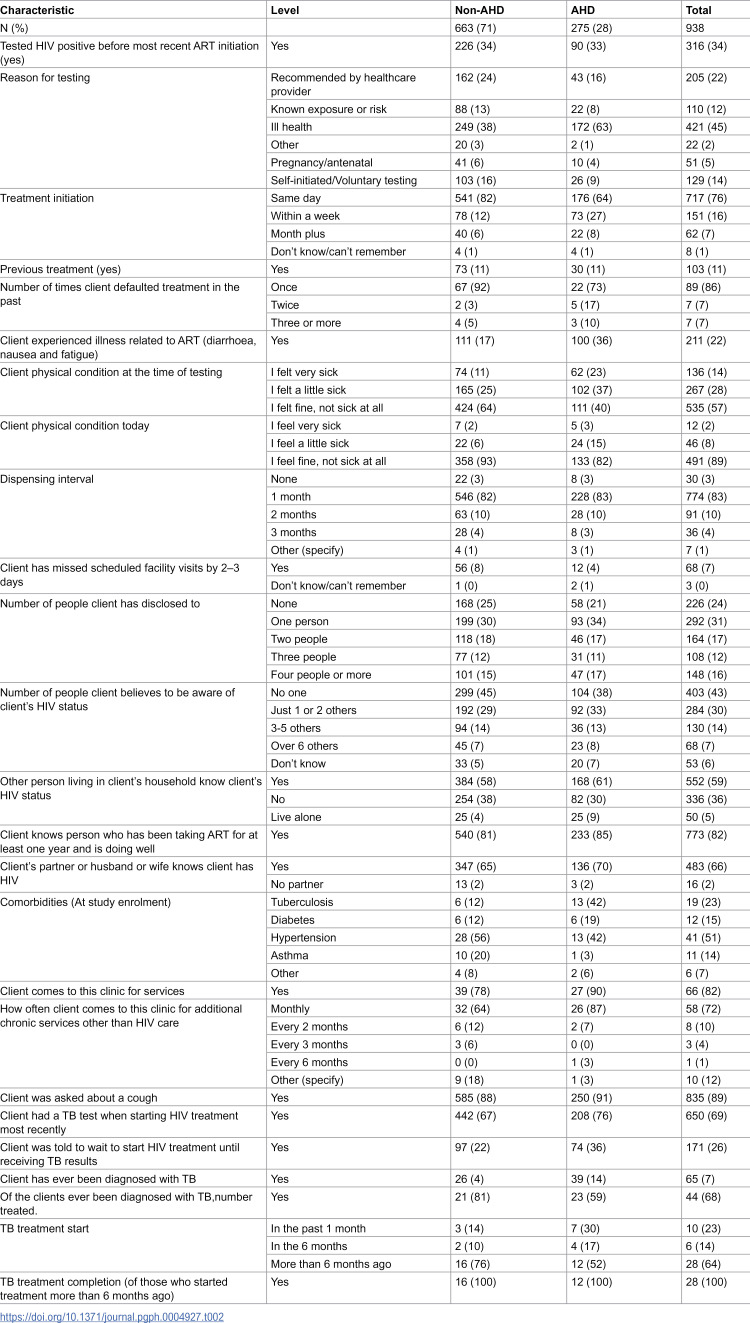
Despite advances in antiretroviral therapy (ART), a notable proportion of individuals still present with advanced HIV disease (AHD) at treatment initiation, defined by CD4 < 200 cells/µL or WHO stage 3/4. This group experiences higher mortality and more opportunistic infections. While guidelines exist, they often do not address AHD clients specific needs early in treatment. Addressing these gaps could improve outcomes. Between September 2022 and June 2023, we surveyed a sequential sample of clients initiating ART or ≤6 months post-initiation at 18 primary healthcare facilities across three provinces. This observational cohort collected socio-demographic data, HIV care history, and service delivery preferences, and linked surveys to routine medical records and described client characteristics using descriptive statistics. Relative risks and risk differences compared outcomes between AHD and non-AHD clients. Primary outcomes were 6-month retention and viral load suppression. Of 1,098 clients (72% female, median age 33), 938 had CD4 or WHO staging at ART start. Of these, 29% (n = 275) had AHD, with a median CD4 of 108 cells/µL. AHD clients were more often male (44% vs. 21%), older (median age: 38 vs. 31 years), and sought care due to illness (63% vs. 33%). TB diagnosis (42% vs. 12%) and testing (76% vs. 67%) were higher. Service preferences and health resource use were similar. Retention at 6 months was similar (80% vs. 75%), but mortality was higher in AHD clients (1.0% vs. 0.2%). AHD clients had more low-level viremia (24% vs. 11%; RR = 2.27, 95% CI = 1.67-3.09) and slightly lower suppression (43% vs. 47%). AHD remains a key barrier to optimal ART outcomes. Clients with AHD experienced poorer viral suppression, despite similar retention rates highlighting the need for early detection, tailored clinical support, and strengthened monitoring. Updating ART guidelines to address AHD-specific needs is critical to improving outcomes in this high-risk population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


