Jiseok Lee, Sang Yoon Kim, Hyoung Woo Chang, Jae Hang Lee, Jun Sung Kim, Sang Hon Park, Kay-Hyun Park, Joon Chul Jung
{"title":"急性A型主动脉夹层院间死亡率的决定因素","authors":"Jiseok Lee, Sang Yoon Kim, Hyoung Woo Chang, Jae Hang Lee, Jun Sung Kim, Sang Hon Park, Kay-Hyun Park, Joon Chul Jung","doi":"10.1093/icvts/ivaf218","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the impact of preoperative characteristics and interhospital distance on interhospital mortality in patients with acute type A aortic dissection.</p><p><strong>Methods: </strong>Patients with acute type A aortic dissection referred to our institution for emergency surgery between May 2020 and December 2024 were retrospectively reviewed. Preoperative characteristics were obtained from registry data based on information available at the time of referral. Interhospital distance was measured in kilometres and minutes using a navigation application.</p><p><strong>Results: </strong>Among 176 patients, 14 interhospital mortalities (8.0%) occurred after the transfer request, with a median interhospital distance of 47 minutes. Significant risk factors for interhospital mortality included pericardial effusion (odds ratio [OR]: 4.03; 95% CI: 1.29-12.64), shock (OR: 97.84; 95% CI: 12.11-790.65), and cardiopulmonary resuscitation before referral (OR: 64.40; 95% CI: 6.57-631.20). Compared to patients referred from the hospitals located within 40 minutes, those referred from the hospitals within 40-80 minutes had a significantly higher risk of interhospital mortality (OR: 6.08; 95% CI: 1.39-42.2). In patients with shock, the cumulative incidence of cardiopulmonary resuscitation increased over time, reaching 21.9% at 60 minutes and 39.0% at 120 minutes after the referral request.</p><p><strong>Conclusions: </strong>Pericardial effusion, shock, cardiopulmonary resuscitation before referral, and interhospital distance were identified as significant risk factors for interhospital mortality in patients with acute type A aortic dissection.</p>","PeriodicalId":73406,"journal":{"name":"Interdisciplinary cardiovascular and thoracic surgery","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12503226/pdf/","citationCount":"0","resultStr":"{\"title\":\"Determinants of Interhospital Mortality in Acute Type A Aortic Dissection.\",\"authors\":\"Jiseok Lee, Sang Yoon Kim, Hyoung Woo Chang, Jae Hang Lee, Jun Sung Kim, Sang Hon Park, Kay-Hyun Park, Joon Chul Jung\",\"doi\":\"10.1093/icvts/ivaf218\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objectives: </strong>To evaluate the impact of preoperative characteristics and interhospital distance on interhospital mortality in patients with acute type A aortic dissection.</p><p><strong>Methods: </strong>Patients with acute type A aortic dissection referred to our institution for emergency surgery between May 2020 and December 2024 were retrospectively reviewed. Preoperative characteristics were obtained from registry data based on information available at the time of referral. Interhospital distance was measured in kilometres and minutes using a navigation application.</p><p><strong>Results: </strong>Among 176 patients, 14 interhospital mortalities (8.0%) occurred after the transfer request, with a median interhospital distance of 47 minutes. Significant risk factors for interhospital mortality included pericardial effusion (odds ratio [OR]: 4.03; 95% CI: 1.29-12.64), shock (OR: 97.84; 95% CI: 12.11-790.65), and cardiopulmonary resuscitation before referral (OR: 64.40; 95% CI: 6.57-631.20). Compared to patients referred from the hospitals located within 40 minutes, those referred from the hospitals within 40-80 minutes had a significantly higher risk of interhospital mortality (OR: 6.08; 95% CI: 1.39-42.2). In patients with shock, the cumulative incidence of cardiopulmonary resuscitation increased over time, reaching 21.9% at 60 minutes and 39.0% at 120 minutes after the referral request.</p><p><strong>Conclusions: </strong>Pericardial effusion, shock, cardiopulmonary resuscitation before referral, and interhospital distance were identified as significant risk factors for interhospital mortality in patients with acute type A aortic dissection.</p>\",\"PeriodicalId\":73406,\"journal\":{\"name\":\"Interdisciplinary cardiovascular and thoracic surgery\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-10-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12503226/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Interdisciplinary cardiovascular and thoracic surgery\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/icvts/ivaf218\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"0\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Interdisciplinary cardiovascular and thoracic surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/icvts/ivaf218","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"0","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Determinants of Interhospital Mortality in Acute Type A Aortic Dissection.
Objectives: To evaluate the impact of preoperative characteristics and interhospital distance on interhospital mortality in patients with acute type A aortic dissection.
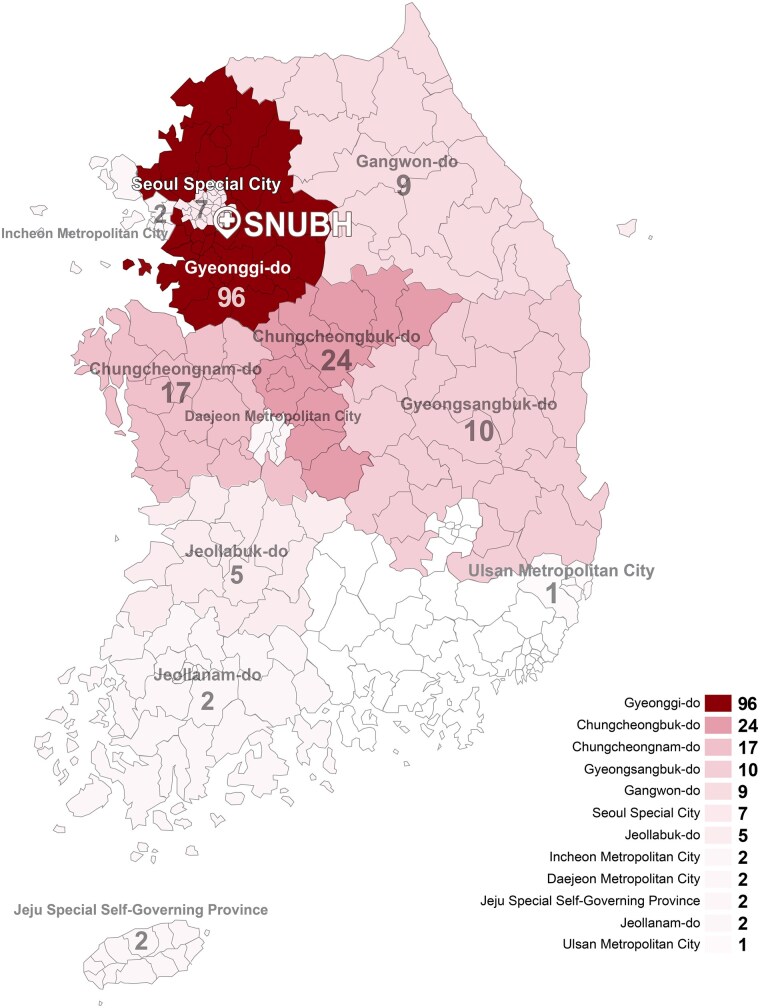
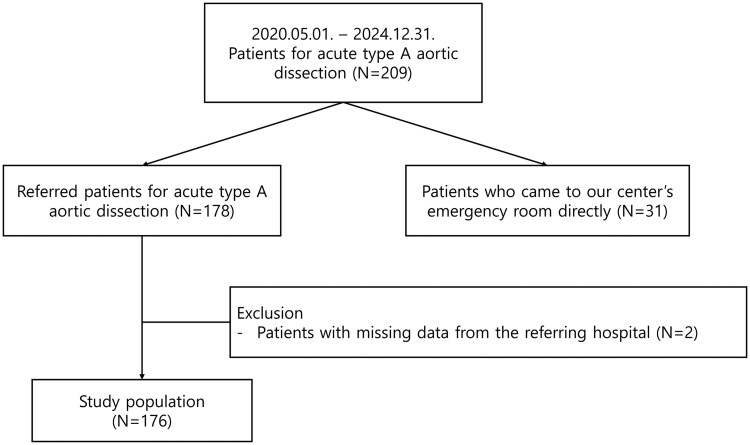
Methods: Patients with acute type A aortic dissection referred to our institution for emergency surgery between May 2020 and December 2024 were retrospectively reviewed. Preoperative characteristics were obtained from registry data based on information available at the time of referral. Interhospital distance was measured in kilometres and minutes using a navigation application.
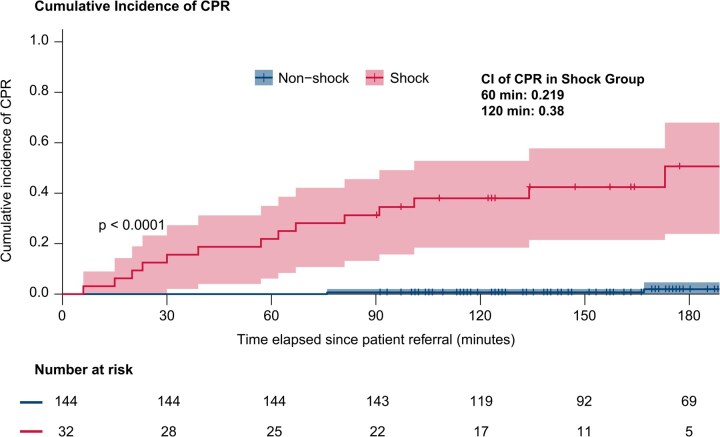
Results: Among 176 patients, 14 interhospital mortalities (8.0%) occurred after the transfer request, with a median interhospital distance of 47 minutes. Significant risk factors for interhospital mortality included pericardial effusion (odds ratio [OR]: 4.03; 95% CI: 1.29-12.64), shock (OR: 97.84; 95% CI: 12.11-790.65), and cardiopulmonary resuscitation before referral (OR: 64.40; 95% CI: 6.57-631.20). Compared to patients referred from the hospitals located within 40 minutes, those referred from the hospitals within 40-80 minutes had a significantly higher risk of interhospital mortality (OR: 6.08; 95% CI: 1.39-42.2). In patients with shock, the cumulative incidence of cardiopulmonary resuscitation increased over time, reaching 21.9% at 60 minutes and 39.0% at 120 minutes after the referral request.
Conclusions: Pericardial effusion, shock, cardiopulmonary resuscitation before referral, and interhospital distance were identified as significant risk factors for interhospital mortality in patients with acute type A aortic dissection.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


