Sebastian Johannes Bauer, Moritz Benjamin Immohr, Friederike Irmgard Schoettler, Yukiharu Sugimura, Arash Mehdiani, Matthias Thielmann, Ajay Moza, Anna Fischbach, Michael Knapen, Evangelos Karasimos, Georg Eberhardt, Gereon Schaelte, Rolf Rossaint, Gernot Marx, Payam Akhyari
{"title":"微创心脏手术快速拔管:4年单中心分析的局限性和教训。","authors":"Sebastian Johannes Bauer, Moritz Benjamin Immohr, Friederike Irmgard Schoettler, Yukiharu Sugimura, Arash Mehdiani, Matthias Thielmann, Ajay Moza, Anna Fischbach, Michael Knapen, Evangelos Karasimos, Georg Eberhardt, Gereon Schaelte, Rolf Rossaint, Gernot Marx, Payam Akhyari","doi":"10.3389/fcvm.2025.1567533","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Fast-track extubation is a key component of the interdisciplinary treatment concept Enhanced Recovery After Surgery (ERAS). In preparation for implementing ERAS as a comprehensive approach, we aimed to analyze the current state of fast-track extubation in the operating room, focusing on Minimally Invasive Cardiac Surgery (MICS). Specifically, we assessed the potential benefits of immediate on-table extubation compared to extubation within six hours after the completion of MICS.</p><p><strong>Methods: </strong>During a 4-year period from 2019-2023, a total of <i>n</i> = 146 patients underwent MICS at our institution. Surgical aspects were retrospectively analysed along with patients' risk profiles and relevant comorbidities. After 1:1 best neighbor propensity score matching, patients who were admitted to intensive care unit intubated but were extubated within six hours after surgery (fast-track, FT) were compared to those who were extubated in the operating room (extubation in tabula, EIT). The primary endpoint was fast-track failure (FTF), a composite of setbacks in the postoperative course: revision surgery, re-intubation, and readmission to ICU or intermediate care unit (IMC).</p><p><strong>Results: </strong>Patients had a median age of 61 years (IQR: 51.3-67.8) and were predominantly male (76.7%). The primary study endpoint occurred in 20.0% of all matched patients (FT: 26.7%, EIT: 13.3%; <i>p</i> = 0.289). FT patients had longer cardiopulmonary bypass times [FT 165.0 min (146.5-217.5); EIT 158.5 min (128.0-189.5); <i>p</i> = 0.047], but the duration of surgery was comparable. Additionally, the average length of hospital stay did not differ. A multivariate analysis was conducted and identified preoperative atrial fibrillation and intraoperative hypothermia as predictive risk factors for FTF.</p><p><strong>Conclusions: </strong>According to our retrospective single-center analysis, extubation in the operating room is feasible and safe even outside of a structured ERAS program. However, as itself it does not impact the further hospital stay, if there is no action thereafter, e.g., same day physiotherapy.</p>","PeriodicalId":12414,"journal":{"name":"Frontiers in Cardiovascular Medicine","volume":"12 ","pages":"1567533"},"PeriodicalIF":2.8000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450875/pdf/","citationCount":"0","resultStr":"{\"title\":\"Fast-track extubation in minimally invasive cardiac surgery: limits and lessons of a 4-year single-center analysis.\",\"authors\":\"Sebastian Johannes Bauer, Moritz Benjamin Immohr, Friederike Irmgard Schoettler, Yukiharu Sugimura, Arash Mehdiani, Matthias Thielmann, Ajay Moza, Anna Fischbach, Michael Knapen, Evangelos Karasimos, Georg Eberhardt, Gereon Schaelte, Rolf Rossaint, Gernot Marx, Payam Akhyari\",\"doi\":\"10.3389/fcvm.2025.1567533\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Fast-track extubation is a key component of the interdisciplinary treatment concept Enhanced Recovery After Surgery (ERAS). In preparation for implementing ERAS as a comprehensive approach, we aimed to analyze the current state of fast-track extubation in the operating room, focusing on Minimally Invasive Cardiac Surgery (MICS). Specifically, we assessed the potential benefits of immediate on-table extubation compared to extubation within six hours after the completion of MICS.</p><p><strong>Methods: </strong>During a 4-year period from 2019-2023, a total of <i>n</i> = 146 patients underwent MICS at our institution. Surgical aspects were retrospectively analysed along with patients' risk profiles and relevant comorbidities. After 1:1 best neighbor propensity score matching, patients who were admitted to intensive care unit intubated but were extubated within six hours after surgery (fast-track, FT) were compared to those who were extubated in the operating room (extubation in tabula, EIT). The primary endpoint was fast-track failure (FTF), a composite of setbacks in the postoperative course: revision surgery, re-intubation, and readmission to ICU or intermediate care unit (IMC).</p><p><strong>Results: </strong>Patients had a median age of 61 years (IQR: 51.3-67.8) and were predominantly male (76.7%). The primary study endpoint occurred in 20.0% of all matched patients (FT: 26.7%, EIT: 13.3%; <i>p</i> = 0.289). FT patients had longer cardiopulmonary bypass times [FT 165.0 min (146.5-217.5); EIT 158.5 min (128.0-189.5); <i>p</i> = 0.047], but the duration of surgery was comparable. Additionally, the average length of hospital stay did not differ. A multivariate analysis was conducted and identified preoperative atrial fibrillation and intraoperative hypothermia as predictive risk factors for FTF.</p><p><strong>Conclusions: </strong>According to our retrospective single-center analysis, extubation in the operating room is feasible and safe even outside of a structured ERAS program. However, as itself it does not impact the further hospital stay, if there is no action thereafter, e.g., same day physiotherapy.</p>\",\"PeriodicalId\":12414,\"journal\":{\"name\":\"Frontiers in Cardiovascular Medicine\",\"volume\":\"12 \",\"pages\":\"1567533\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450875/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Cardiovascular Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fcvm.2025.1567533\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Cardiovascular Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fcvm.2025.1567533","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
背景:快速拔管是跨学科治疗理念的关键组成部分,促进术后恢复(ERAS)。为了准备实施ERAS作为一种综合方法,我们旨在分析手术室快速通道拔管的现状,重点是微创心脏手术(MICS)。具体地说,我们评估了与MICS完成后6小时内拔管相比,立即在台上拔管的潜在益处。方法:在2019-2023年的4年期间,共有n = 146例患者在我院接受了MICS。回顾性分析手术方面以及患者的风险概况和相关合并症。在1:1最佳邻居倾向评分匹配后,将入院重症监护病房插管但术后6小时内拔管的患者(快速通道,FT)与在手术室拔管的患者(tabula拔管,EIT)进行比较。主要终点是快速通道失败(FTF),这是术后过程中一系列挫折的综合:翻修手术、重新插管、再入ICU或中间护理病房(IMC)。结果:患者中位年龄61岁(IQR: 51.3-67.8),以男性为主(76.7%)。主要研究终点发生在所有匹配患者的20.0% (FT: 26.7%, EIT: 13.3%; p = 0.289)。FT患者体外循环次数较长[FT = 165.0 min (146.5 ~ 217.5);EIT 158.5 min (128.0-189.5);P = 0.047],但手术时间具有可比性。此外,平均住院时间没有差异。进行了多因素分析,确定术前心房颤动和术中低温是FTF的预测危险因素。结论:根据我们的回顾性单中心分析,即使在结构化的ERAS计划之外,在手术室拔管也是可行且安全的。但是,如果此后没有采取任何行动,例如当天物理治疗,则其本身不影响进一步住院。
Fast-track extubation in minimally invasive cardiac surgery: limits and lessons of a 4-year single-center analysis.
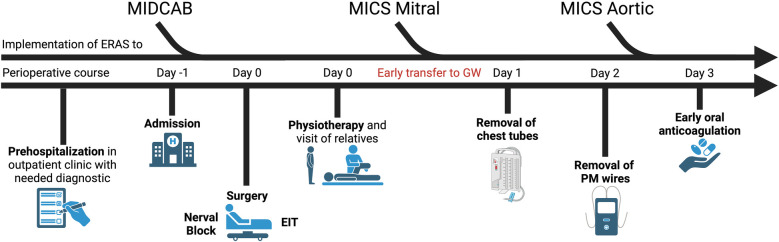
Background: Fast-track extubation is a key component of the interdisciplinary treatment concept Enhanced Recovery After Surgery (ERAS). In preparation for implementing ERAS as a comprehensive approach, we aimed to analyze the current state of fast-track extubation in the operating room, focusing on Minimally Invasive Cardiac Surgery (MICS). Specifically, we assessed the potential benefits of immediate on-table extubation compared to extubation within six hours after the completion of MICS.
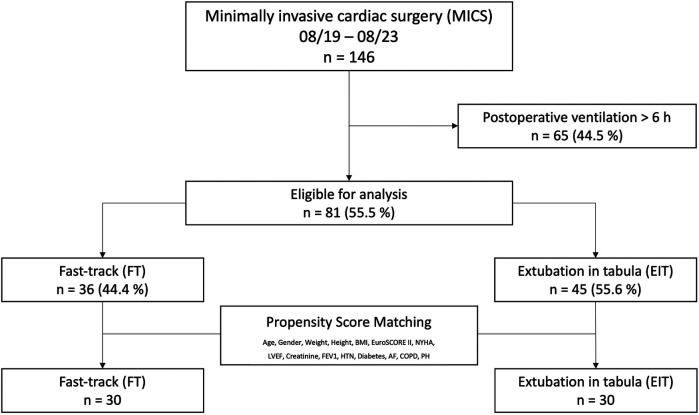
Methods: During a 4-year period from 2019-2023, a total of n = 146 patients underwent MICS at our institution. Surgical aspects were retrospectively analysed along with patients' risk profiles and relevant comorbidities. After 1:1 best neighbor propensity score matching, patients who were admitted to intensive care unit intubated but were extubated within six hours after surgery (fast-track, FT) were compared to those who were extubated in the operating room (extubation in tabula, EIT). The primary endpoint was fast-track failure (FTF), a composite of setbacks in the postoperative course: revision surgery, re-intubation, and readmission to ICU or intermediate care unit (IMC).
Results: Patients had a median age of 61 years (IQR: 51.3-67.8) and were predominantly male (76.7%). The primary study endpoint occurred in 20.0% of all matched patients (FT: 26.7%, EIT: 13.3%; p = 0.289). FT patients had longer cardiopulmonary bypass times [FT 165.0 min (146.5-217.5); EIT 158.5 min (128.0-189.5); p = 0.047], but the duration of surgery was comparable. Additionally, the average length of hospital stay did not differ. A multivariate analysis was conducted and identified preoperative atrial fibrillation and intraoperative hypothermia as predictive risk factors for FTF.
Conclusions: According to our retrospective single-center analysis, extubation in the operating room is feasible and safe even outside of a structured ERAS program. However, as itself it does not impact the further hospital stay, if there is no action thereafter, e.g., same day physiotherapy.
期刊介绍:
Frontiers? Which frontiers? Where exactly are the frontiers of cardiovascular medicine? And who should be defining these frontiers?
At Frontiers in Cardiovascular Medicine we believe it is worth being curious to foresee and explore beyond the current frontiers. In other words, we would like, through the articles published by our community journal Frontiers in Cardiovascular Medicine, to anticipate the future of cardiovascular medicine, and thus better prevent cardiovascular disorders and improve therapeutic options and outcomes of our patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


