Niels A Stens, Geert A A Versteeg, Maxim J P Rooijakkers, Roos de Lange, Stijn J H Bonekamp, Marleen H van Wely, Robert Jan M van Geuns, Michel W A Verkroost, Leen A F M van Garsse, Guillaume S C Geuzebroek, Robin H Heijmen, Lokien X van Nunen, Dick H J Thijssen, Niels van Royen
{"title":"经导管主动脉瓣置换术中有创测量血流动力学自动评估的构建有效性。","authors":"Niels A Stens, Geert A A Versteeg, Maxim J P Rooijakkers, Roos de Lange, Stijn J H Bonekamp, Marleen H van Wely, Robert Jan M van Geuns, Michel W A Verkroost, Leen A F M van Garsse, Guillaume S C Geuzebroek, Robin H Heijmen, Lokien X van Nunen, Dick H J Thijssen, Niels van Royen","doi":"10.1093/ehjdh/ztaf069","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Paravalvular regurgitation (PVR) is frequently observed following Transcatheter Aortic Valve Replacement (TAVR). Periprocedural monitoring of invasive hemodynamics has shown promise for diagnosis of PVR, but automated software options are lacking. We aimed to develop a rule-based algorithm for automated assessment of hemodynamic indices of PVR, and evaluate its construct validity and discriminatory value for cardiac magnetic resonance (CMR)-derived relevant PVR compared to standard manual hemodynamic assessment.</p><p><strong>Methods and results: </strong>Left ventricular and aortic pressures were invasively measured during TAVR using fluid-filled pigtail catheters. To evaluate construct validity of automated vs. manual assessment of invasive hemodynamics, we compared (i) proportion of cardiac cycles affected by arrhythmias/noise, (ii) pressure gradients, and (iii) PVR indices. Additionally, we compared the discriminatory value of automatically and manually determined PVR indices for CMR-determined relevant PVR at 30-days. In total, 77 patients were enrolled (664 cardiac cycles). Automated filtering of cardiac cycles affected by arrhythmias/noise had a high sensitivity (95.2%) and specificity (86.4%). In addition, excellent agreement was observed between automated and manual computation of mean gradients pre- and post-TAVR [39.3 ± 12.1 vs. 37.5 ± 11.9 mmHg, intra-class correlation coefficient (ICC): 0.916; 1.92 ± 5.87 vs. 1.14 ± 5.89, ICC: 0.957, respectively], and PVR indices [diastolic delta (DD): 41.7 ± 12.4 vs. 40.6 ± 12.3 mmHg, ICC: 0.982, respectively]. Automated and manual assessment of DD showed comparable discriminatory value for relevant PVR [area under the curve (AUC): 0.81 vs. 0.80, respectively].</p><p><strong>Conclusion: </strong>Rule-based, automated assessment of hemodynamic indices of PVR showed excellent construct validity and discriminatory value for CMR-determined relevant PVR, supporting its use for real-time evaluation and risk stratification in TAVR patients.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 5","pages":"1006-1014"},"PeriodicalIF":4.4000,"publicationDate":"2025-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450506/pdf/","citationCount":"0","resultStr":"{\"title\":\"Construct validity of automated assessment of invasively measured hemodynamics during transcatheter aortic valve replacement.\",\"authors\":\"Niels A Stens, Geert A A Versteeg, Maxim J P Rooijakkers, Roos de Lange, Stijn J H Bonekamp, Marleen H van Wely, Robert Jan M van Geuns, Michel W A Verkroost, Leen A F M van Garsse, Guillaume S C Geuzebroek, Robin H Heijmen, Lokien X van Nunen, Dick H J Thijssen, Niels van Royen\",\"doi\":\"10.1093/ehjdh/ztaf069\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Paravalvular regurgitation (PVR) is frequently observed following Transcatheter Aortic Valve Replacement (TAVR). Periprocedural monitoring of invasive hemodynamics has shown promise for diagnosis of PVR, but automated software options are lacking. We aimed to develop a rule-based algorithm for automated assessment of hemodynamic indices of PVR, and evaluate its construct validity and discriminatory value for cardiac magnetic resonance (CMR)-derived relevant PVR compared to standard manual hemodynamic assessment.</p><p><strong>Methods and results: </strong>Left ventricular and aortic pressures were invasively measured during TAVR using fluid-filled pigtail catheters. To evaluate construct validity of automated vs. manual assessment of invasive hemodynamics, we compared (i) proportion of cardiac cycles affected by arrhythmias/noise, (ii) pressure gradients, and (iii) PVR indices. Additionally, we compared the discriminatory value of automatically and manually determined PVR indices for CMR-determined relevant PVR at 30-days. In total, 77 patients were enrolled (664 cardiac cycles). Automated filtering of cardiac cycles affected by arrhythmias/noise had a high sensitivity (95.2%) and specificity (86.4%). In addition, excellent agreement was observed between automated and manual computation of mean gradients pre- and post-TAVR [39.3 ± 12.1 vs. 37.5 ± 11.9 mmHg, intra-class correlation coefficient (ICC): 0.916; 1.92 ± 5.87 vs. 1.14 ± 5.89, ICC: 0.957, respectively], and PVR indices [diastolic delta (DD): 41.7 ± 12.4 vs. 40.6 ± 12.3 mmHg, ICC: 0.982, respectively]. Automated and manual assessment of DD showed comparable discriminatory value for relevant PVR [area under the curve (AUC): 0.81 vs. 0.80, respectively].</p><p><strong>Conclusion: </strong>Rule-based, automated assessment of hemodynamic indices of PVR showed excellent construct validity and discriminatory value for CMR-determined relevant PVR, supporting its use for real-time evaluation and risk stratification in TAVR patients.</p>\",\"PeriodicalId\":72965,\"journal\":{\"name\":\"European heart journal. Digital health\",\"volume\":\"6 5\",\"pages\":\"1006-1014\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-06-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450506/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjdh/ztaf069\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf069","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
摘要
目的:经导管主动脉瓣置换术(TAVR)后经常观察到瓣旁反流(PVR)。围手术期监测侵入性血流动力学已显示出诊断PVR的希望,但缺乏自动化的软件选择。我们旨在开发一种基于规则的PVR血流动力学指标自动评估算法,并与标准手工血流动力学评估相比,评估其对心脏磁共振(CMR)衍生相关PVR的结构效度和区分价值。方法和结果:在TAVR期间,使用充满液体的细尾导管有创地测量左心室和主动脉压力。为了评估侵入性血流动力学自动评估与人工评估的结构有效性,我们比较了(i)心律失常/噪声影响的心周期比例,(ii)压力梯度和(iii) PVR指数。此外,我们比较了自动和手动确定的PVR指标在30天cmr确定的相关PVR的区别值。共纳入77例患者(664个心动周期)。心律失常/噪声影响的心循环自动过滤具有高灵敏度(95.2%)和特异性(86.4%)。此外,自动和手动计算tavr前后的平均梯度之间的一致性非常好[39.3±12.1 vs 37.5±11.9 mmHg,类内相关系数(ICC): 0.916;1.92±5.87比1.14±5.89,ICC分别为0.957],PVR指数[舒张δ (DD): 41.7±12.4比40.6±12.3 mmHg, ICC分别为0.982]。自动和手动DD评估对相关PVR的区分值相当[曲线下面积(AUC)分别为0.81和0.80]。结论:基于规则的PVR血流动力学指标自动评估对cmr确定的相关PVR具有良好的结构效度和判别价值,支持其用于TAVR患者的实时评估和风险分层。
Construct validity of automated assessment of invasively measured hemodynamics during transcatheter aortic valve replacement.
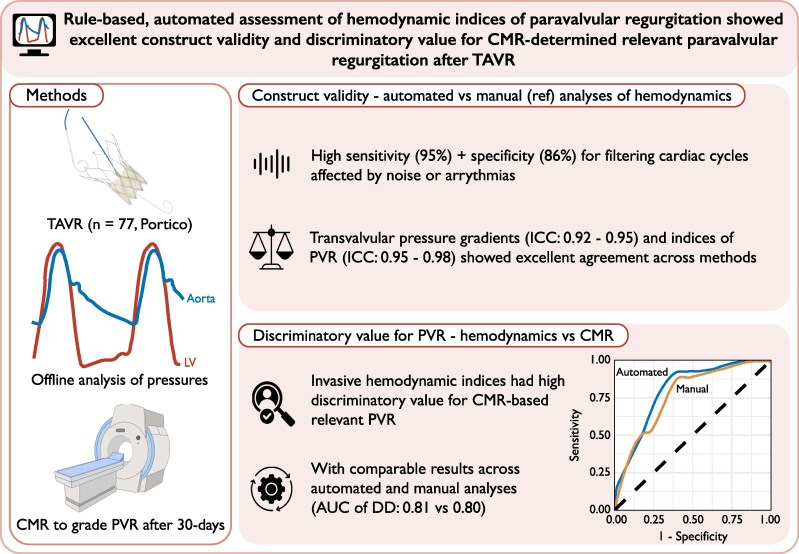
Aims: Paravalvular regurgitation (PVR) is frequently observed following Transcatheter Aortic Valve Replacement (TAVR). Periprocedural monitoring of invasive hemodynamics has shown promise for diagnosis of PVR, but automated software options are lacking. We aimed to develop a rule-based algorithm for automated assessment of hemodynamic indices of PVR, and evaluate its construct validity and discriminatory value for cardiac magnetic resonance (CMR)-derived relevant PVR compared to standard manual hemodynamic assessment.
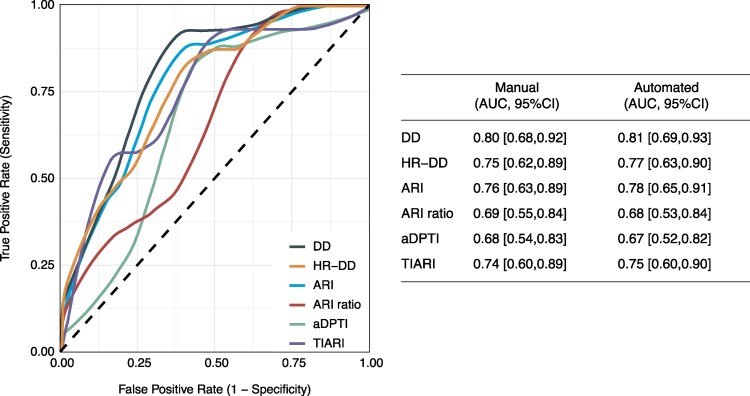
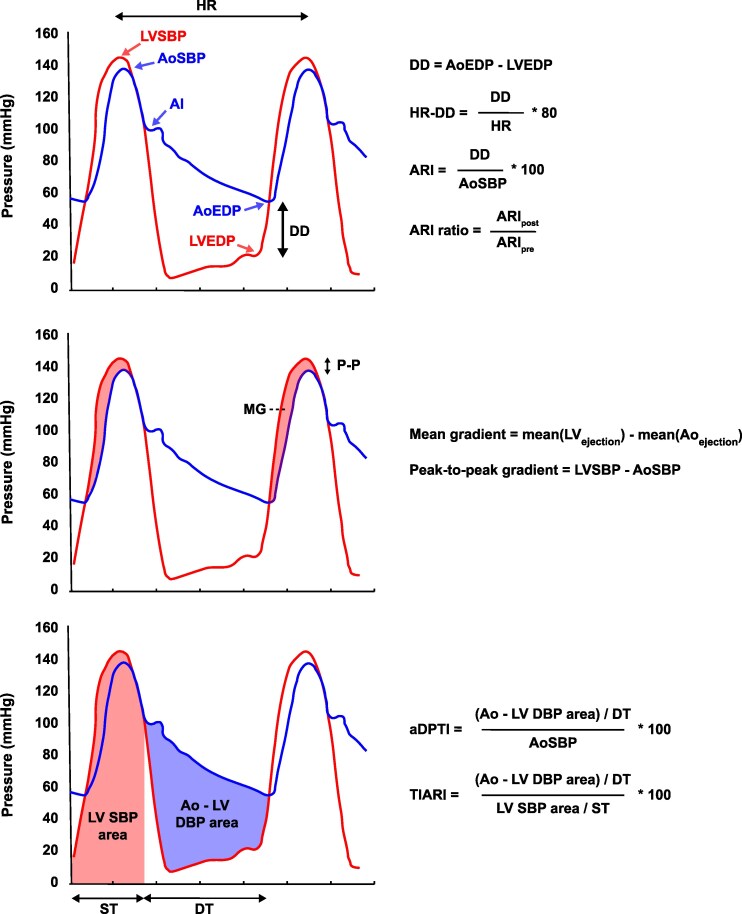
Methods and results: Left ventricular and aortic pressures were invasively measured during TAVR using fluid-filled pigtail catheters. To evaluate construct validity of automated vs. manual assessment of invasive hemodynamics, we compared (i) proportion of cardiac cycles affected by arrhythmias/noise, (ii) pressure gradients, and (iii) PVR indices. Additionally, we compared the discriminatory value of automatically and manually determined PVR indices for CMR-determined relevant PVR at 30-days. In total, 77 patients were enrolled (664 cardiac cycles). Automated filtering of cardiac cycles affected by arrhythmias/noise had a high sensitivity (95.2%) and specificity (86.4%). In addition, excellent agreement was observed between automated and manual computation of mean gradients pre- and post-TAVR [39.3 ± 12.1 vs. 37.5 ± 11.9 mmHg, intra-class correlation coefficient (ICC): 0.916; 1.92 ± 5.87 vs. 1.14 ± 5.89, ICC: 0.957, respectively], and PVR indices [diastolic delta (DD): 41.7 ± 12.4 vs. 40.6 ± 12.3 mmHg, ICC: 0.982, respectively]. Automated and manual assessment of DD showed comparable discriminatory value for relevant PVR [area under the curve (AUC): 0.81 vs. 0.80, respectively].
Conclusion: Rule-based, automated assessment of hemodynamic indices of PVR showed excellent construct validity and discriminatory value for CMR-determined relevant PVR, supporting its use for real-time evaluation and risk stratification in TAVR patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


