Olof Persson Lindell, Martin Henriksson, Lars O Karlsson, Staffan Nilsson, Emmanouil Charitakis, Magnus Janzon
{"title":"心房颤动临床决策支持系统的成本效益:一项基于随机对照试验的建模研究。","authors":"Olof Persson Lindell, Martin Henriksson, Lars O Karlsson, Staffan Nilsson, Emmanouil Charitakis, Magnus Janzon","doi":"10.1093/ehjdh/ztaf087","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Atrial fibrillation (AF) is a common arrythmia that increases the risk of thromboembolism. Despite the effectiveness of anticoagulation in AF, underuse remains a substantial problem. Clinical decision support (CDS) systems may increase adherence to guideline recommended anticoagulation in AF. However, evidence regarding the cost-effectiveness of these interventions is lacking. The aim of this study was therefore to evaluate the cost-effectiveness of a CDS for AF.</p><p><strong>Methods and results: </strong>We developed a disease progression model with a Markov structure and simulated a cohort of hypothetical individuals with AF through a standard of care and a CDS strategy. The adherence to anticoagulation in the model was based on the treatment effect reported in the CDS-AF trial, which evaluated the effect of a CDS in patients with AF in the primary care in Östergötland, Sweden. The cost-effectiveness of the CDS-AF intervention compared with standard of care was determined by estimating costs and quality-adjusted life years (QALYs) gained over a lifetime time horizon and was reported as an incremental cost-effectiveness ratio (ICER) assessed against a decision-threshold of €50 000. Uncertainty was evaluated using both one-way and probabilistic sensitivity analysis (PSA). The CDS-intervention resulted in fewer ischaemic strokes but more bleedings. The mean per patient gain in QALYs was 0.012 and the ICER was €963 per QALY gained. The result of the PSA indicated a high probability that the ICER was below €50 000.</p><p><strong>Conclusion: </strong>The CDS intervention used in the CDS-AF trial appears to yield health gains at a lower cost than typically considered cost-effective.</p><p><strong>Trial registration: </strong>NCT02635685.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"6 5","pages":"997-1005"},"PeriodicalIF":4.4000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450513/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness of a clinical decision support system for atrial fibrillation: an RCT-based modelling study.\",\"authors\":\"Olof Persson Lindell, Martin Henriksson, Lars O Karlsson, Staffan Nilsson, Emmanouil Charitakis, Magnus Janzon\",\"doi\":\"10.1093/ehjdh/ztaf087\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Atrial fibrillation (AF) is a common arrythmia that increases the risk of thromboembolism. Despite the effectiveness of anticoagulation in AF, underuse remains a substantial problem. Clinical decision support (CDS) systems may increase adherence to guideline recommended anticoagulation in AF. However, evidence regarding the cost-effectiveness of these interventions is lacking. The aim of this study was therefore to evaluate the cost-effectiveness of a CDS for AF.</p><p><strong>Methods and results: </strong>We developed a disease progression model with a Markov structure and simulated a cohort of hypothetical individuals with AF through a standard of care and a CDS strategy. The adherence to anticoagulation in the model was based on the treatment effect reported in the CDS-AF trial, which evaluated the effect of a CDS in patients with AF in the primary care in Östergötland, Sweden. The cost-effectiveness of the CDS-AF intervention compared with standard of care was determined by estimating costs and quality-adjusted life years (QALYs) gained over a lifetime time horizon and was reported as an incremental cost-effectiveness ratio (ICER) assessed against a decision-threshold of €50 000. Uncertainty was evaluated using both one-way and probabilistic sensitivity analysis (PSA). The CDS-intervention resulted in fewer ischaemic strokes but more bleedings. The mean per patient gain in QALYs was 0.012 and the ICER was €963 per QALY gained. The result of the PSA indicated a high probability that the ICER was below €50 000.</p><p><strong>Conclusion: </strong>The CDS intervention used in the CDS-AF trial appears to yield health gains at a lower cost than typically considered cost-effective.</p><p><strong>Trial registration: </strong>NCT02635685.</p>\",\"PeriodicalId\":72965,\"journal\":{\"name\":\"European heart journal. Digital health\",\"volume\":\"6 5\",\"pages\":\"997-1005\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2025-08-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12450513/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjdh/ztaf087\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztaf087","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Cost-effectiveness of a clinical decision support system for atrial fibrillation: an RCT-based modelling study.
Aims: Atrial fibrillation (AF) is a common arrythmia that increases the risk of thromboembolism. Despite the effectiveness of anticoagulation in AF, underuse remains a substantial problem. Clinical decision support (CDS) systems may increase adherence to guideline recommended anticoagulation in AF. However, evidence regarding the cost-effectiveness of these interventions is lacking. The aim of this study was therefore to evaluate the cost-effectiveness of a CDS for AF.
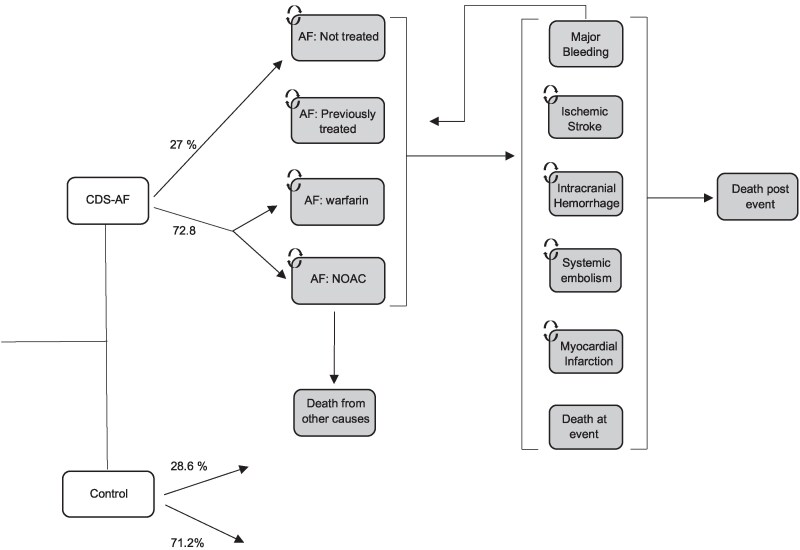
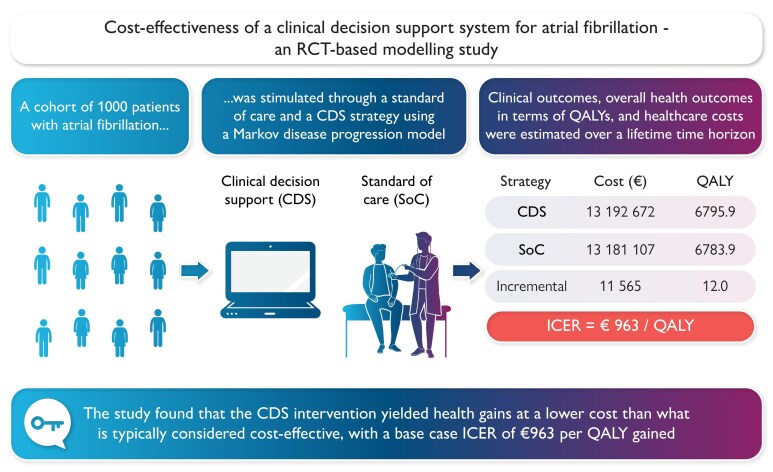
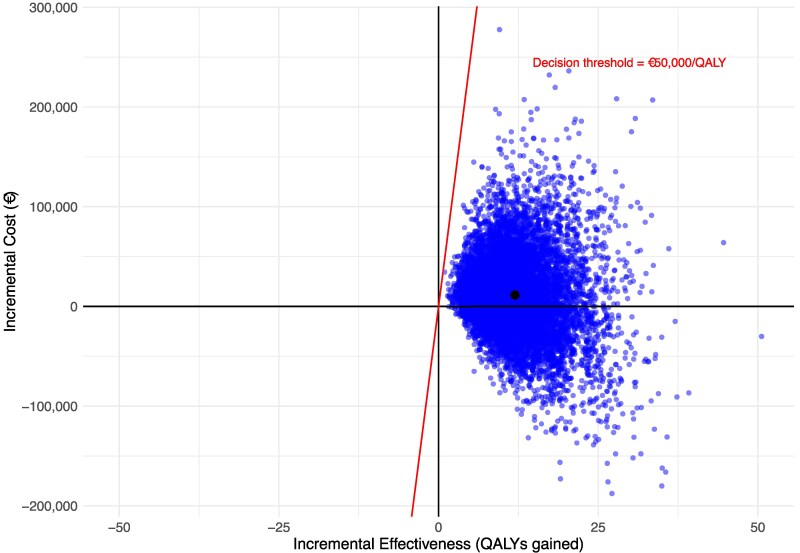
Methods and results: We developed a disease progression model with a Markov structure and simulated a cohort of hypothetical individuals with AF through a standard of care and a CDS strategy. The adherence to anticoagulation in the model was based on the treatment effect reported in the CDS-AF trial, which evaluated the effect of a CDS in patients with AF in the primary care in Östergötland, Sweden. The cost-effectiveness of the CDS-AF intervention compared with standard of care was determined by estimating costs and quality-adjusted life years (QALYs) gained over a lifetime time horizon and was reported as an incremental cost-effectiveness ratio (ICER) assessed against a decision-threshold of €50 000. Uncertainty was evaluated using both one-way and probabilistic sensitivity analysis (PSA). The CDS-intervention resulted in fewer ischaemic strokes but more bleedings. The mean per patient gain in QALYs was 0.012 and the ICER was €963 per QALY gained. The result of the PSA indicated a high probability that the ICER was below €50 000.
Conclusion: The CDS intervention used in the CDS-AF trial appears to yield health gains at a lower cost than typically considered cost-effective.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


