Makomo Makazu, Kazuya Koizumi, Jun Kubota, Karen Kimura, Sakue Masuda
{"title":"应用钻孔扩张器经肿瘤硬道经乳头引流胰液渗漏1例报告。","authors":"Makomo Makazu, Kazuya Koizumi, Jun Kubota, Karen Kimura, Sakue Masuda","doi":"10.4253/wjge.v17.i9.110424","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pancreatic fluid leakage is a rare complication of pancreatic cancer and often requires drainage when conservative therapy fails. Endoscopic, percutaneous, and surgical drainage are options. Minimally invasive endoscopic procedures are generally considered the first-line treatment, with either a transpapillary approach or an endoscopic ultrasound-guided transmural approach selected depending on the case. Various dilators are used to dilate tracts to the leakage site. However, reports of dilation through a rigid trans-tumoral tract using a drill dilator remain extremely rare.</p><p><strong>Case summary: </strong>A 74-year-old woman with pancreatic body and tail cancer developed fever and left-sided chest pain after multiple courses of chemotherapy. Computed tomography revealed fluid accumulation around the pancreatic tail and spleen along with a left pleural effusion. The effusion was diagnosed as reactive secondary to pancreatic fluid leakage. Endoscopic retrograde cholangiopancreatography identified irregular stenosis of the main pancreatic duct in the pancreatic body. Distal to the stenosis, the main ductal structure was nearly obliterated by the tumor. The contrast medium had leaked into the pancreatic fluid leakage area through several fine, disrupted ductal structures. The guidewire was successfully advanced through an extremely fine tract that was not the main contrast-filling route. Standard dilators failed to expand the rigid trans-tumoral tract. A second endoscopic retrograde cholangiopancreatography using a drill dilator successfully expanded the trans-tumoral tract, enabling endoscopic nasopancreatic drainage tube placement. Subsequently, the pancreatic fluid leakage and pleural effusion resolved.</p><p><strong>Conclusion: </strong>Even in rigid trans-tumoral tracts, the use of a drill dilator can facilitate successful tract expansion, enabling effective drainage.</p>","PeriodicalId":23953,"journal":{"name":"World Journal of Gastrointestinal Endoscopy","volume":"17 9","pages":"110424"},"PeriodicalIF":1.8000,"publicationDate":"2025-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12444271/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transpapillary drainage of pancreatic fluid leakage <i>via</i> a rigid trans-tumoral tract using a drill dilator: A case report.\",\"authors\":\"Makomo Makazu, Kazuya Koizumi, Jun Kubota, Karen Kimura, Sakue Masuda\",\"doi\":\"10.4253/wjge.v17.i9.110424\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pancreatic fluid leakage is a rare complication of pancreatic cancer and often requires drainage when conservative therapy fails. Endoscopic, percutaneous, and surgical drainage are options. Minimally invasive endoscopic procedures are generally considered the first-line treatment, with either a transpapillary approach or an endoscopic ultrasound-guided transmural approach selected depending on the case. Various dilators are used to dilate tracts to the leakage site. However, reports of dilation through a rigid trans-tumoral tract using a drill dilator remain extremely rare.</p><p><strong>Case summary: </strong>A 74-year-old woman with pancreatic body and tail cancer developed fever and left-sided chest pain after multiple courses of chemotherapy. Computed tomography revealed fluid accumulation around the pancreatic tail and spleen along with a left pleural effusion. The effusion was diagnosed as reactive secondary to pancreatic fluid leakage. Endoscopic retrograde cholangiopancreatography identified irregular stenosis of the main pancreatic duct in the pancreatic body. Distal to the stenosis, the main ductal structure was nearly obliterated by the tumor. The contrast medium had leaked into the pancreatic fluid leakage area through several fine, disrupted ductal structures. The guidewire was successfully advanced through an extremely fine tract that was not the main contrast-filling route. Standard dilators failed to expand the rigid trans-tumoral tract. A second endoscopic retrograde cholangiopancreatography using a drill dilator successfully expanded the trans-tumoral tract, enabling endoscopic nasopancreatic drainage tube placement. Subsequently, the pancreatic fluid leakage and pleural effusion resolved.</p><p><strong>Conclusion: </strong>Even in rigid trans-tumoral tracts, the use of a drill dilator can facilitate successful tract expansion, enabling effective drainage.</p>\",\"PeriodicalId\":23953,\"journal\":{\"name\":\"World Journal of Gastrointestinal Endoscopy\",\"volume\":\"17 9\",\"pages\":\"110424\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2025-09-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12444271/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4253/wjge.v17.i9.110424\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4253/wjge.v17.i9.110424","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Transpapillary drainage of pancreatic fluid leakage via a rigid trans-tumoral tract using a drill dilator: A case report.
Background: Pancreatic fluid leakage is a rare complication of pancreatic cancer and often requires drainage when conservative therapy fails. Endoscopic, percutaneous, and surgical drainage are options. Minimally invasive endoscopic procedures are generally considered the first-line treatment, with either a transpapillary approach or an endoscopic ultrasound-guided transmural approach selected depending on the case. Various dilators are used to dilate tracts to the leakage site. However, reports of dilation through a rigid trans-tumoral tract using a drill dilator remain extremely rare.
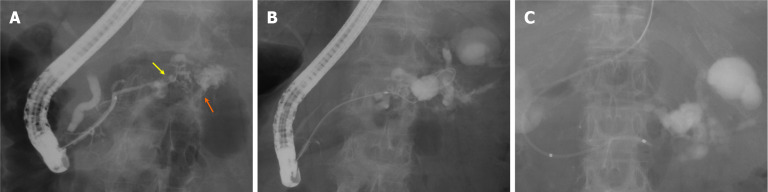
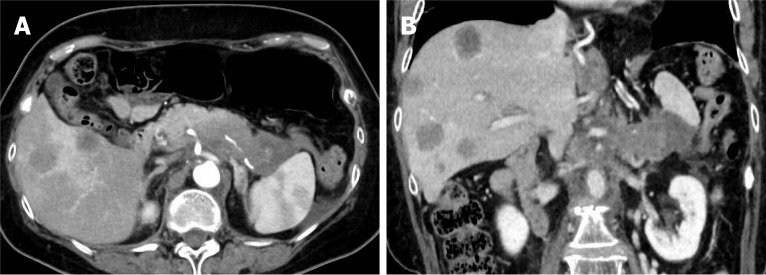
Case summary: A 74-year-old woman with pancreatic body and tail cancer developed fever and left-sided chest pain after multiple courses of chemotherapy. Computed tomography revealed fluid accumulation around the pancreatic tail and spleen along with a left pleural effusion. The effusion was diagnosed as reactive secondary to pancreatic fluid leakage. Endoscopic retrograde cholangiopancreatography identified irregular stenosis of the main pancreatic duct in the pancreatic body. Distal to the stenosis, the main ductal structure was nearly obliterated by the tumor. The contrast medium had leaked into the pancreatic fluid leakage area through several fine, disrupted ductal structures. The guidewire was successfully advanced through an extremely fine tract that was not the main contrast-filling route. Standard dilators failed to expand the rigid trans-tumoral tract. A second endoscopic retrograde cholangiopancreatography using a drill dilator successfully expanded the trans-tumoral tract, enabling endoscopic nasopancreatic drainage tube placement. Subsequently, the pancreatic fluid leakage and pleural effusion resolved.
Conclusion: Even in rigid trans-tumoral tracts, the use of a drill dilator can facilitate successful tract expansion, enabling effective drainage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


