Xue Shen, Pei Chen, Lijun Liu, Sufang Shi, Xujie Zhou, Sean J Barbour, Jicheng Lv, Hong Zhang
{"title":"新疗法改善了IgAN的预后,限制了国际IgA肾病预测工具的适用性。","authors":"Xue Shen, Pei Chen, Lijun Liu, Sufang Shi, Xujie Zhou, Sean J Barbour, Jicheng Lv, Hong Zhang","doi":"10.1093/ckj/sfaf251","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The International IgA Nephropathy Prediction Tools using clinical variables and the Oxford MEST scores were developed in outdated cohorts. External validation is required to assess the tool's applicability in predicting progression risk for patients on novel therapies.</p><p><strong>Methods: </strong>We included 677 immunoglobulin A nephropathy (IgAN) patients (Peking University First Hospital, 2003-23) treated with endothelin receptor antagonists, Nefecon, sodium-glucose cotransporter 2 inhibitors, hydroxychloroquine or telitacicept, a BAFF/APRIL inhibitor. The primary outcome was defined as a 50% decline in estimated glomerular filtration rate or end-stage kidney disease. Discrimination (C-statistic), calibration [calibration slope, Integrated Calibration Index (ICI)], model fit (R<sup>2</sup> <sub>D</sub>) and risk stratification (Kaplan-Meier curves) were assessed.</p><p><strong>Results: </strong>The median follow-up was 4.8 years (interquartile range 2.2, 8.1), and 190 (28.1%) patients experienced the primary outcome, with a 5-year risk of 9.8%. Compared with the median biopsy year of reported cohorts of original model, our cohort is more contemporary (2017). We validated both original and updated models (and for full model with and without race version). All versions showed adequate discrimination, poor calibration and model fit: C-statistic ∼0.74, calibration slope ∼0.50, R<sup>2</sup> <sub>D</sub> <20%, ICI >0.10, and poor separation of Kaplan-Meier curves, except for the highest-risk group. The tools consistently overestimated risk in patients receiving novel therapies. These findings further demonstrated that novel therapies can improved clinical outcomes for IgAN patients.</p><p><strong>Conclusions: </strong>In this study, both versions of both models demonstrated limited performance and overestimated risks. Given the prognostic improvement with novel IgAN therapies, these prediction tools may need updating for use in currently treated patients.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 9","pages":"sfaf251"},"PeriodicalIF":4.6000,"publicationDate":"2025-08-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445651/pdf/","citationCount":"0","resultStr":"{\"title\":\"Novel therapies improve prognosis of IgAN and limit the applicability of the International IgA Nephropathy Prediction Tool.\",\"authors\":\"Xue Shen, Pei Chen, Lijun Liu, Sufang Shi, Xujie Zhou, Sean J Barbour, Jicheng Lv, Hong Zhang\",\"doi\":\"10.1093/ckj/sfaf251\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The International IgA Nephropathy Prediction Tools using clinical variables and the Oxford MEST scores were developed in outdated cohorts. External validation is required to assess the tool's applicability in predicting progression risk for patients on novel therapies.</p><p><strong>Methods: </strong>We included 677 immunoglobulin A nephropathy (IgAN) patients (Peking University First Hospital, 2003-23) treated with endothelin receptor antagonists, Nefecon, sodium-glucose cotransporter 2 inhibitors, hydroxychloroquine or telitacicept, a BAFF/APRIL inhibitor. The primary outcome was defined as a 50% decline in estimated glomerular filtration rate or end-stage kidney disease. Discrimination (C-statistic), calibration [calibration slope, Integrated Calibration Index (ICI)], model fit (R<sup>2</sup> <sub>D</sub>) and risk stratification (Kaplan-Meier curves) were assessed.</p><p><strong>Results: </strong>The median follow-up was 4.8 years (interquartile range 2.2, 8.1), and 190 (28.1%) patients experienced the primary outcome, with a 5-year risk of 9.8%. Compared with the median biopsy year of reported cohorts of original model, our cohort is more contemporary (2017). We validated both original and updated models (and for full model with and without race version). All versions showed adequate discrimination, poor calibration and model fit: C-statistic ∼0.74, calibration slope ∼0.50, R<sup>2</sup> <sub>D</sub> <20%, ICI >0.10, and poor separation of Kaplan-Meier curves, except for the highest-risk group. The tools consistently overestimated risk in patients receiving novel therapies. These findings further demonstrated that novel therapies can improved clinical outcomes for IgAN patients.</p><p><strong>Conclusions: </strong>In this study, both versions of both models demonstrated limited performance and overestimated risks. Given the prognostic improvement with novel IgAN therapies, these prediction tools may need updating for use in currently treated patients.</p>\",\"PeriodicalId\":10435,\"journal\":{\"name\":\"Clinical Kidney Journal\",\"volume\":\"18 9\",\"pages\":\"sfaf251\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-08-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12445651/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Kidney Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ckj/sfaf251\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf251","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:使用临床变量和牛津MEST评分的国际IgA肾病预测工具是在过时的队列中开发的。需要外部验证来评估该工具在预测新疗法患者进展风险方面的适用性。方法:纳入2003-23年北京大学第一医院677例免疫球蛋白A肾病(IgAN)患者,采用内皮素受体拮抗剂、Nefecon、钠-葡萄糖共转运蛋白2抑制剂、羟氯喹或BAFF/APRIL抑制剂替利他塞普治疗。主要终点被定义为肾小球滤过率估计下降50%或终末期肾病。评估辨别力(C-statistic)、校正[校正斜率、综合校正指数(ICI)]、模型拟合(R2 D)和风险分层(Kaplan-Meier曲线)。结果:中位随访时间为4.8年(四分位数范围2.2,8.1),190例(28.1%)患者出现主要结局,5年风险为9.8%。与原始模型报告队列的中位活检年份相比,我们的队列更现代(2017年)。我们验证了原始和更新的模型(以及带有和不带有种族版本的完整模型)。除了最高风险组外,所有版本均表现出足够的鉴别性,校正和模型拟合较差:c -统计量~ 0.74,校正斜率~ 0.50,R2 D 0.10, Kaplan-Meier曲线分离较差。这些工具始终高估了接受新疗法的患者的风险。这些发现进一步表明,新疗法可以改善IgAN患者的临床结果。结论:在本研究中,两种模型的两个版本都表现出有限的性能和高估的风险。鉴于新型IgAN疗法的预后改善,这些预测工具可能需要更新以用于目前接受治疗的患者。
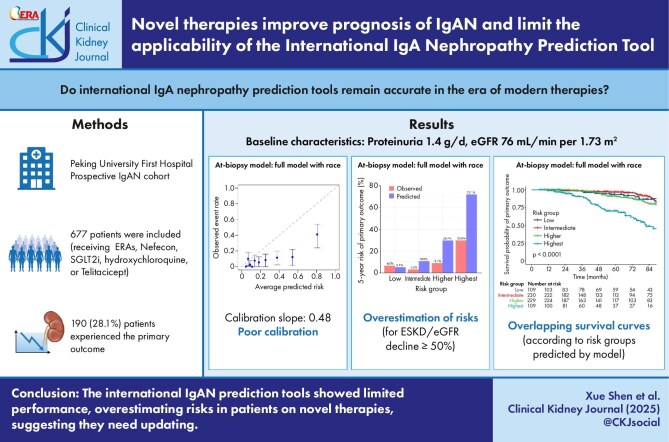
Novel therapies improve prognosis of IgAN and limit the applicability of the International IgA Nephropathy Prediction Tool.
Background: The International IgA Nephropathy Prediction Tools using clinical variables and the Oxford MEST scores were developed in outdated cohorts. External validation is required to assess the tool's applicability in predicting progression risk for patients on novel therapies.
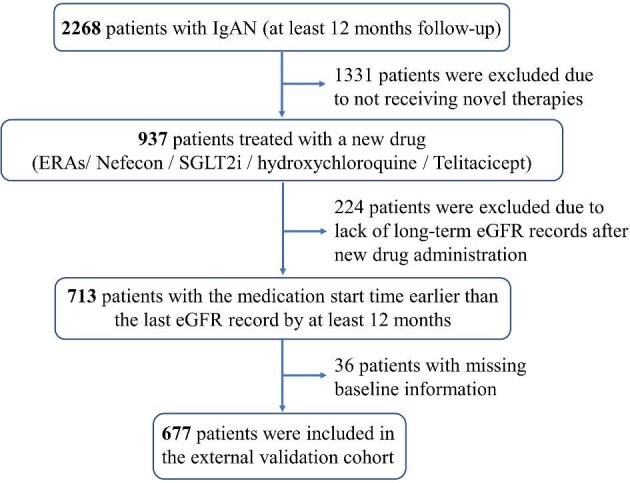
Methods: We included 677 immunoglobulin A nephropathy (IgAN) patients (Peking University First Hospital, 2003-23) treated with endothelin receptor antagonists, Nefecon, sodium-glucose cotransporter 2 inhibitors, hydroxychloroquine or telitacicept, a BAFF/APRIL inhibitor. The primary outcome was defined as a 50% decline in estimated glomerular filtration rate or end-stage kidney disease. Discrimination (C-statistic), calibration [calibration slope, Integrated Calibration Index (ICI)], model fit (R2D) and risk stratification (Kaplan-Meier curves) were assessed.
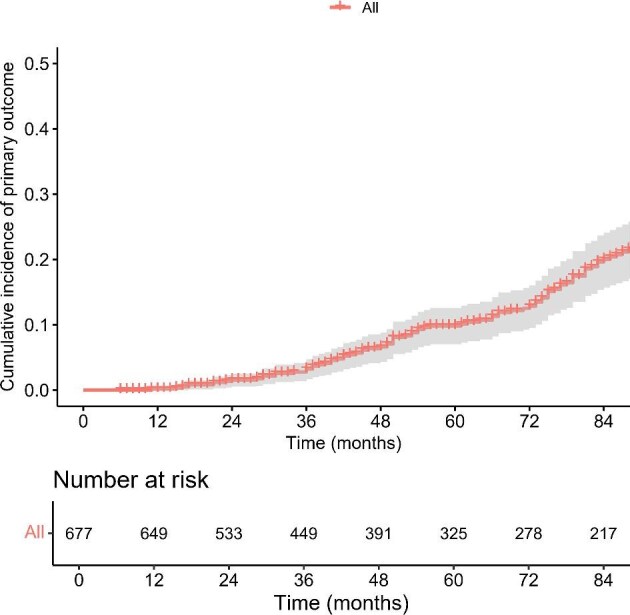
Results: The median follow-up was 4.8 years (interquartile range 2.2, 8.1), and 190 (28.1%) patients experienced the primary outcome, with a 5-year risk of 9.8%. Compared with the median biopsy year of reported cohorts of original model, our cohort is more contemporary (2017). We validated both original and updated models (and for full model with and without race version). All versions showed adequate discrimination, poor calibration and model fit: C-statistic ∼0.74, calibration slope ∼0.50, R2D <20%, ICI >0.10, and poor separation of Kaplan-Meier curves, except for the highest-risk group. The tools consistently overestimated risk in patients receiving novel therapies. These findings further demonstrated that novel therapies can improved clinical outcomes for IgAN patients.
Conclusions: In this study, both versions of both models demonstrated limited performance and overestimated risks. Given the prognostic improvement with novel IgAN therapies, these prediction tools may need updating for use in currently treated patients.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


