{"title":"IPDMA - RADICAL - NSCLC:个体参与者数据荟萃分析和系统评价局部根治性治疗低转移性NSCLC。","authors":"Krishna Tiwari, Muhammad Aaqib Shamim, Isha Yadav, Rakesh Dodiya, Ajay Kumar Kondeti, Naveen Dutt, Parmod Kumar, Sonali Kar, Vikas Tiwari, Pradeep Dwivedi, Surjit Singh, Shoban Babu Varthya","doi":"10.1136/bmjresp-2025-003276","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The role of radical local therapy in oligometastatic non-small cell lung cancer (NSCLC) is rapidly evolving and has shown mixed results. We assessed the effect of add-on radical local therapy versus systemic therapy alone on overall survival (OS), progression-free survival (PFS) and safety in oligometastatic NSCLC.</p><p><strong>Methods: </strong>In this systematic review and individual participant data (IPD) meta-analysis, we screened PubMed, Embase, Scopus and CENTRAL until 20 April 2025 for randomised controlled trials (RCTs) answering our research question. We retrieved IPD from survival curves of published reports and used one-stage IPD meta-analysis. We also estimated the more clinically intuitive restricted mean survival time difference (RMSTD). We assessed between-study heterogeneity using the median HR (MHR). We assessed risk of bias using the Risk of Bias 2 tool and rated the evidence certainty using the Grading of Recommendations, Assessment, Development and Evaluations framework.</p><p><strong>Findings: </strong>We screened 1004 records to include ten RCTs (mostly at a low risk of bias) with 752 participants (338 males), predominantly using radiotherapy as radical local therapy. Add-on radical local therapy improved OS by 38% [HR: 0.62, 95% CI 0.50 to 0.76; high certainty of evidence]. Between-trial heterogeneity does not affect the results, only leading to 3% difference [MHR 1.03]. Add-on radical local therapy leads to longer OS by 0.47 month (0.21-0.72), 2.18 months (0.74-3.63), 4.20 months (1.95-6.45) and 6.65 months (4.05-9.24) over 1, 2, 3 and 4 years. Add-on radical local therapy possibly improved PFS by 40% (HR: 0.60, 95% CI 0.45 to 0.80; low certainty of evidence). Radical local therapy was well tolerated with no major safety concerns.</p><p><strong>Interpretation: </strong>Add-on radical local therapy-chiefly radiotherapy-is beneficial in oligometastatic NSCLC. Inconsistent reporting of safety limited quantitative synthesis. Future studies may address the role of surgery as radical local therapy, and the role of programmed death ligand 1 expression.</p><p><strong>Prospero registration number: </strong>CRD42024576829.</p>","PeriodicalId":9048,"journal":{"name":"BMJ Open Respiratory Research","volume":"12 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2025-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12458624/pdf/","citationCount":"0","resultStr":"{\"title\":\"IPDMA - RADICAL - NSCLC: individual participant data meta-analysis and systematic review of radical local therapy for oligometastatic NSCLC.\",\"authors\":\"Krishna Tiwari, Muhammad Aaqib Shamim, Isha Yadav, Rakesh Dodiya, Ajay Kumar Kondeti, Naveen Dutt, Parmod Kumar, Sonali Kar, Vikas Tiwari, Pradeep Dwivedi, Surjit Singh, Shoban Babu Varthya\",\"doi\":\"10.1136/bmjresp-2025-003276\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The role of radical local therapy in oligometastatic non-small cell lung cancer (NSCLC) is rapidly evolving and has shown mixed results. We assessed the effect of add-on radical local therapy versus systemic therapy alone on overall survival (OS), progression-free survival (PFS) and safety in oligometastatic NSCLC.</p><p><strong>Methods: </strong>In this systematic review and individual participant data (IPD) meta-analysis, we screened PubMed, Embase, Scopus and CENTRAL until 20 April 2025 for randomised controlled trials (RCTs) answering our research question. We retrieved IPD from survival curves of published reports and used one-stage IPD meta-analysis. We also estimated the more clinically intuitive restricted mean survival time difference (RMSTD). We assessed between-study heterogeneity using the median HR (MHR). We assessed risk of bias using the Risk of Bias 2 tool and rated the evidence certainty using the Grading of Recommendations, Assessment, Development and Evaluations framework.</p><p><strong>Findings: </strong>We screened 1004 records to include ten RCTs (mostly at a low risk of bias) with 752 participants (338 males), predominantly using radiotherapy as radical local therapy. Add-on radical local therapy improved OS by 38% [HR: 0.62, 95% CI 0.50 to 0.76; high certainty of evidence]. Between-trial heterogeneity does not affect the results, only leading to 3% difference [MHR 1.03]. Add-on radical local therapy leads to longer OS by 0.47 month (0.21-0.72), 2.18 months (0.74-3.63), 4.20 months (1.95-6.45) and 6.65 months (4.05-9.24) over 1, 2, 3 and 4 years. Add-on radical local therapy possibly improved PFS by 40% (HR: 0.60, 95% CI 0.45 to 0.80; low certainty of evidence). Radical local therapy was well tolerated with no major safety concerns.</p><p><strong>Interpretation: </strong>Add-on radical local therapy-chiefly radiotherapy-is beneficial in oligometastatic NSCLC. Inconsistent reporting of safety limited quantitative synthesis. Future studies may address the role of surgery as radical local therapy, and the role of programmed death ligand 1 expression.</p><p><strong>Prospero registration number: </strong>CRD42024576829.</p>\",\"PeriodicalId\":9048,\"journal\":{\"name\":\"BMJ Open Respiratory Research\",\"volume\":\"12 1\",\"pages\":\"\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2025-09-17\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12458624/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMJ Open Respiratory Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/bmjresp-2025-003276\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjresp-2025-003276","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
摘要
局部根治性治疗在低转移性非小细胞肺癌(NSCLC)中的作用正在迅速发展,并显示出不同的结果。我们评估了加治局部根治性治疗与单独全身治疗在低转移性NSCLC总生存期(OS)、无进展生存期(PFS)和安全性方面的影响。方法:在这项系统评价和个体参与者数据(IPD)荟萃分析中,我们筛选了PubMed、Embase、Scopus和CENTRAL,直到2025年4月20日,以寻找回答我们研究问题的随机对照试验(rct)。我们从已发表报告的生存曲线中检索IPD,并使用一期IPD荟萃分析。我们还估计了临床上更直观的限制平均生存时间差异(RMSTD)。我们使用中位HR (MHR)评估研究间异质性。我们使用risk of bias 2工具评估偏倚风险,并使用分级推荐、评估、发展和评估框架对证据确定性进行评级。研究结果:我们筛选了1004项记录,包括10项随机对照试验(大部分为低偏倚风险),752名参与者(338名男性),主要使用放射治疗作为根治性局部治疗。附加根治性局部治疗使OS改善38% [HR: 0.62, 95% CI 0.50 ~ 0.76;证据的高度确定性]。试验间异质性不影响结果,仅导致3%的差异[MHR 1.03]。在1年、2年、3年和4年间,局部根治性治疗的OS延长分别为0.47个月(0.21-0.72)、2.18个月(0.74-3.63)、4.20个月(1.95-6.45)和6.65个月(4.05-9.24)。附加根治性局部治疗可能使PFS提高40% (HR: 0.60, 95% CI 0.45 - 0.80;证据确定性低)。根治性局部治疗耐受性良好,无重大安全问题。结论:局部根治性治疗(主要是放疗)对少转移性非小细胞肺癌是有益的。不一致的安全性报告限制了定量合成。未来的研究可能会探讨手术作为根治性局部治疗的作用,以及程序性死亡配体1表达的作用。普洛斯彼罗注册号:CRD42024576829。
IPDMA - RADICAL - NSCLC: individual participant data meta-analysis and systematic review of radical local therapy for oligometastatic NSCLC.
Introduction: The role of radical local therapy in oligometastatic non-small cell lung cancer (NSCLC) is rapidly evolving and has shown mixed results. We assessed the effect of add-on radical local therapy versus systemic therapy alone on overall survival (OS), progression-free survival (PFS) and safety in oligometastatic NSCLC.
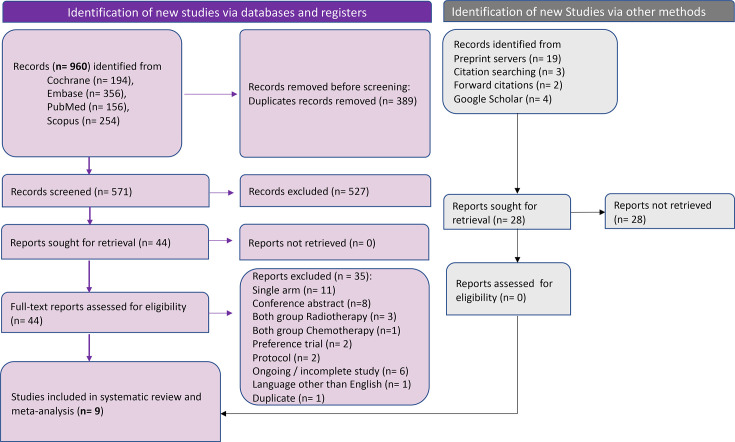
Methods: In this systematic review and individual participant data (IPD) meta-analysis, we screened PubMed, Embase, Scopus and CENTRAL until 20 April 2025 for randomised controlled trials (RCTs) answering our research question. We retrieved IPD from survival curves of published reports and used one-stage IPD meta-analysis. We also estimated the more clinically intuitive restricted mean survival time difference (RMSTD). We assessed between-study heterogeneity using the median HR (MHR). We assessed risk of bias using the Risk of Bias 2 tool and rated the evidence certainty using the Grading of Recommendations, Assessment, Development and Evaluations framework.
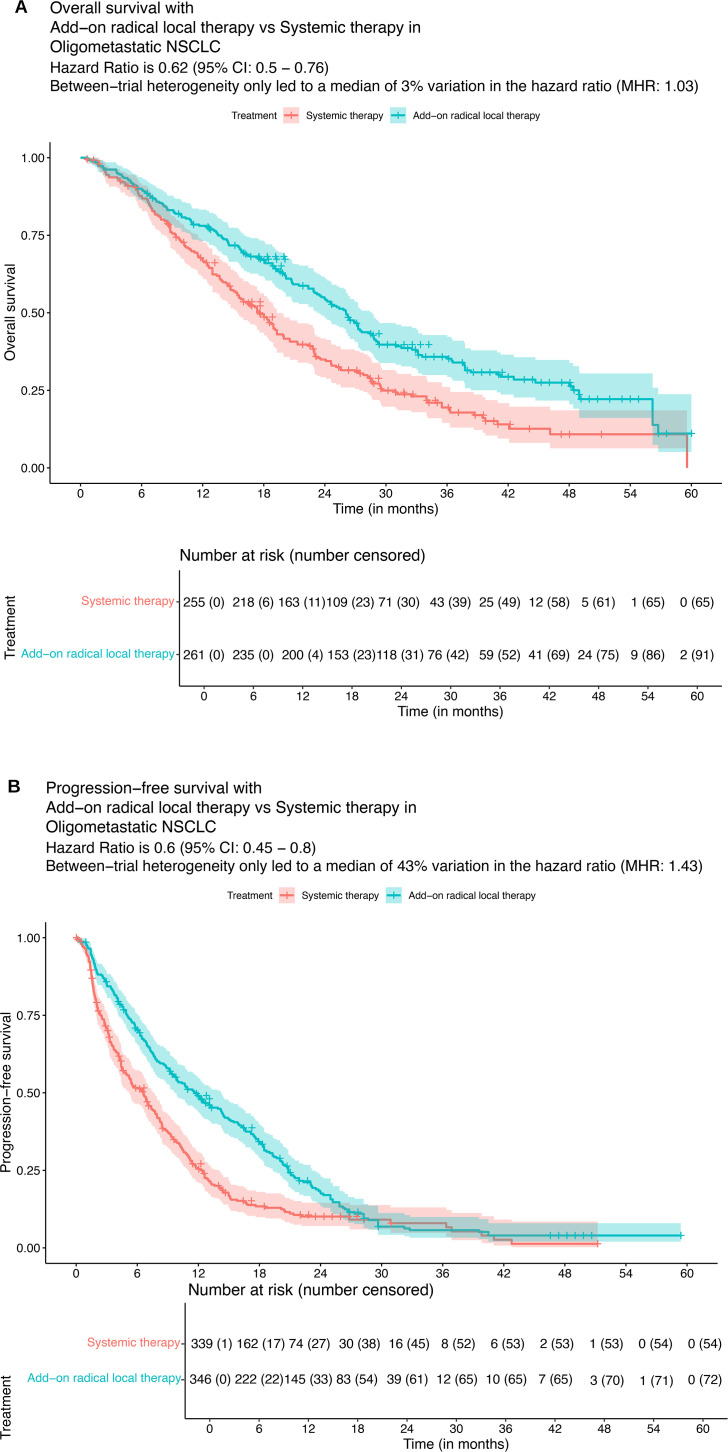
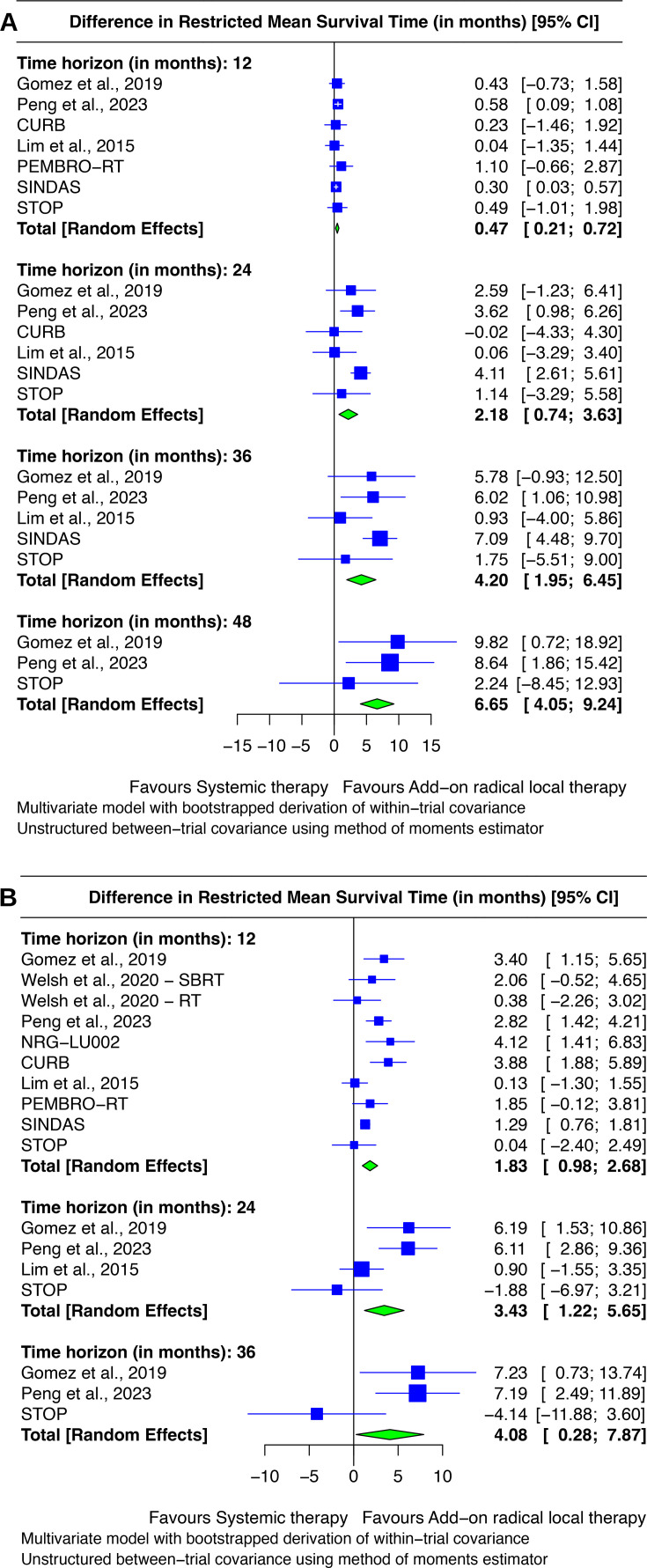
Findings: We screened 1004 records to include ten RCTs (mostly at a low risk of bias) with 752 participants (338 males), predominantly using radiotherapy as radical local therapy. Add-on radical local therapy improved OS by 38% [HR: 0.62, 95% CI 0.50 to 0.76; high certainty of evidence]. Between-trial heterogeneity does not affect the results, only leading to 3% difference [MHR 1.03]. Add-on radical local therapy leads to longer OS by 0.47 month (0.21-0.72), 2.18 months (0.74-3.63), 4.20 months (1.95-6.45) and 6.65 months (4.05-9.24) over 1, 2, 3 and 4 years. Add-on radical local therapy possibly improved PFS by 40% (HR: 0.60, 95% CI 0.45 to 0.80; low certainty of evidence). Radical local therapy was well tolerated with no major safety concerns.
Interpretation: Add-on radical local therapy-chiefly radiotherapy-is beneficial in oligometastatic NSCLC. Inconsistent reporting of safety limited quantitative synthesis. Future studies may address the role of surgery as radical local therapy, and the role of programmed death ligand 1 expression.
期刊介绍:
BMJ Open Respiratory Research is a peer-reviewed, open access journal publishing respiratory and critical care medicine. It is the sister journal to Thorax and co-owned by the British Thoracic Society and BMJ. The journal focuses on robustness of methodology and scientific rigour with less emphasis on novelty or perceived impact. BMJ Open Respiratory Research operates a rapid review process, with continuous publication online, ensuring timely, up-to-date research is available worldwide. The journal publishes review articles and all research study types: Basic science including laboratory based experiments and animal models, Pilot studies or proof of concept, Observational studies, Study protocols, Registries, Clinical trials from phase I to multicentre randomised clinical trials, Systematic reviews and meta-analyses.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


