Silvia Grazietta Foddai, Maria Infantino, Mariangela Manfredi, Francesca Pavia, Maurizio Benucci, Francesca Li Gobbi, Massimo Radin, Irene Cecchi, Alice Barinotti, Savino Sciascia
{"title":"优化抗磷脂抗体测试:现实世界的适当性和资源利用分析。","authors":"Silvia Grazietta Foddai, Maria Infantino, Mariangela Manfredi, Francesca Pavia, Maurizio Benucci, Francesca Li Gobbi, Massimo Radin, Irene Cecchi, Alice Barinotti, Savino Sciascia","doi":"10.1007/s12026-025-09682-x","DOIUrl":null,"url":null,"abstract":"<p><p>Efficient utilization of healthcare resources, including laboratory testing, is crucial for environmental sustainability and cost-effectiveness. The diagnosis of APS requires the presence of at least one clinical event (either an objectively confirmed thrombotic event and/or pregnancy complication) and detection of one or more aPL (lupus anticoagulant [LA], IgG/IgM anticardiolipin [aCL], and/or IgG/IgM anti-β2 glycoprotein-1 [aβ2GPI]). However, inappropriate requests for aPL tests contribute to unnecessary healthcare expenses and environmental impact. This study evaluates the appropriateness of aPL testing in a clinical setting. A retrospective analysis was conducted on 642 patients attending the San Giovanni Di Dio Hospital, Florence (11/2023-02/2024). Diagnostic suspicion underlying aPL test requests were classified as appropriate, inappropriate, or unevaluable using a scoring system based on clinical recommendations. Appropriateness assessment was performed independently by two researchers and reconciled with a third expert. Patient demographics, test results, and the specialty of the physicians ordering aPL were recorded and analyzed. Of the 642 queries, 36% were deemed appropriate, 42% inappropriate, and 22% unevaluable. Family physicians accounted for 53% of all test requests but exhibited the highest rate of inappropriate requests (44%). Rheumatologists, internal medicine physicians, and gynecologists demonstrated better adherence to recommendations (with 34%, 30%, and 18% of inappropriate requests, respectively). Only 4.9% of patients underwent comprehensive aPL testing per international standards (Sidney criteria). Among the 115 aPL-positive cases, multiple antibody positivity was more common in appropriate test requests. Inappropriate requests often stemmed from conditions without established links to APS, such as alopecia, hypercholesterolemia, and dysmenorrhea. A considerable proportion of aPL testing in routine practice lacks clinical justification, reflecting variability in guideline adherence across specialties. Inappropriate testing increases healthcare costs, specialist referrals, and environmental burdens. Improved education, adherence to diagnostic recommendations, and sustainable practices are critical to optimizing APS testing and resource utilization.</p>","PeriodicalId":13389,"journal":{"name":"Immunologic Research","volume":"73 1","pages":"130"},"PeriodicalIF":3.1000,"publicationDate":"2025-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12441101/pdf/","citationCount":"0","resultStr":"{\"title\":\"Optimizing antiphospholipid antibody testing: a real-world analysis of appropriateness and resource utilization.\",\"authors\":\"Silvia Grazietta Foddai, Maria Infantino, Mariangela Manfredi, Francesca Pavia, Maurizio Benucci, Francesca Li Gobbi, Massimo Radin, Irene Cecchi, Alice Barinotti, Savino Sciascia\",\"doi\":\"10.1007/s12026-025-09682-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Efficient utilization of healthcare resources, including laboratory testing, is crucial for environmental sustainability and cost-effectiveness. The diagnosis of APS requires the presence of at least one clinical event (either an objectively confirmed thrombotic event and/or pregnancy complication) and detection of one or more aPL (lupus anticoagulant [LA], IgG/IgM anticardiolipin [aCL], and/or IgG/IgM anti-β2 glycoprotein-1 [aβ2GPI]). However, inappropriate requests for aPL tests contribute to unnecessary healthcare expenses and environmental impact. This study evaluates the appropriateness of aPL testing in a clinical setting. A retrospective analysis was conducted on 642 patients attending the San Giovanni Di Dio Hospital, Florence (11/2023-02/2024). Diagnostic suspicion underlying aPL test requests were classified as appropriate, inappropriate, or unevaluable using a scoring system based on clinical recommendations. Appropriateness assessment was performed independently by two researchers and reconciled with a third expert. Patient demographics, test results, and the specialty of the physicians ordering aPL were recorded and analyzed. Of the 642 queries, 36% were deemed appropriate, 42% inappropriate, and 22% unevaluable. Family physicians accounted for 53% of all test requests but exhibited the highest rate of inappropriate requests (44%). Rheumatologists, internal medicine physicians, and gynecologists demonstrated better adherence to recommendations (with 34%, 30%, and 18% of inappropriate requests, respectively). Only 4.9% of patients underwent comprehensive aPL testing per international standards (Sidney criteria). Among the 115 aPL-positive cases, multiple antibody positivity was more common in appropriate test requests. Inappropriate requests often stemmed from conditions without established links to APS, such as alopecia, hypercholesterolemia, and dysmenorrhea. A considerable proportion of aPL testing in routine practice lacks clinical justification, reflecting variability in guideline adherence across specialties. Inappropriate testing increases healthcare costs, specialist referrals, and environmental burdens. Improved education, adherence to diagnostic recommendations, and sustainable practices are critical to optimizing APS testing and resource utilization.</p>\",\"PeriodicalId\":13389,\"journal\":{\"name\":\"Immunologic Research\",\"volume\":\"73 1\",\"pages\":\"130\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-09-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12441101/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Immunologic Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12026-025-09682-x\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Immunologic Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12026-025-09682-x","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
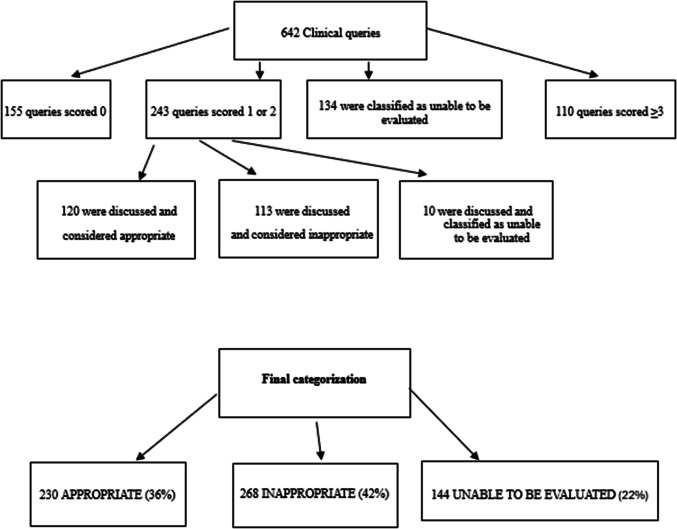
有效利用医疗资源,包括实验室测试,对于环境可持续性和成本效益至关重要。APS的诊断需要出现至少一种临床事件(客观证实的血栓形成事件和/或妊娠并发症),并检测一种或多种aPL(狼疮抗凝剂[LA]、IgG/IgM抗心磷脂[aCL]和/或IgG/IgM抗β2糖蛋白-1 [a -β 2gpi])。然而,不适当的aPL测试请求会造成不必要的医疗保健费用和环境影响。本研究评估aPL检测在临床环境中的适宜性。回顾性分析了在佛罗伦萨San Giovanni Di Dio医院就诊的642例患者(2023年11月至2024年2月)。使用基于临床建议的评分系统,将aPL测试请求的诊断怀疑分类为适当、不适当或不可评估。适当性评估由两名研究人员独立进行,并与第三名专家进行协调。记录和分析患者人口统计数据、检测结果和开具aPL的医生的专业。在642个查询中,36%被认为是合适的,42%是不合适的,22%是不可评估的。家庭医生占所有测试请求的53%,但表现出最高的不适当请求率(44%)。风湿病医生、内科医生和妇科医生对建议的依从性更好(不适当的要求分别为34%、30%和18%)。只有4.9%的患者按照国际标准(悉尼标准)进行了全面的aPL检测。在115例apl阳性病例中,在适当的检测要求中,多抗体阳性更为常见。不适当的要求通常源于与APS没有建立联系的疾病,如脱发、高胆固醇血症和痛经。在常规实践中,相当大比例的aPL检测缺乏临床依据,这反映了不同专业指南依从性的差异。不适当的检测增加了医疗成本、专家转诊和环境负担。改进教育、遵守诊断建议和可持续实践是优化APS测试和资源利用的关键。
Optimizing antiphospholipid antibody testing: a real-world analysis of appropriateness and resource utilization.
Efficient utilization of healthcare resources, including laboratory testing, is crucial for environmental sustainability and cost-effectiveness. The diagnosis of APS requires the presence of at least one clinical event (either an objectively confirmed thrombotic event and/or pregnancy complication) and detection of one or more aPL (lupus anticoagulant [LA], IgG/IgM anticardiolipin [aCL], and/or IgG/IgM anti-β2 glycoprotein-1 [aβ2GPI]). However, inappropriate requests for aPL tests contribute to unnecessary healthcare expenses and environmental impact. This study evaluates the appropriateness of aPL testing in a clinical setting. A retrospective analysis was conducted on 642 patients attending the San Giovanni Di Dio Hospital, Florence (11/2023-02/2024). Diagnostic suspicion underlying aPL test requests were classified as appropriate, inappropriate, or unevaluable using a scoring system based on clinical recommendations. Appropriateness assessment was performed independently by two researchers and reconciled with a third expert. Patient demographics, test results, and the specialty of the physicians ordering aPL were recorded and analyzed. Of the 642 queries, 36% were deemed appropriate, 42% inappropriate, and 22% unevaluable. Family physicians accounted for 53% of all test requests but exhibited the highest rate of inappropriate requests (44%). Rheumatologists, internal medicine physicians, and gynecologists demonstrated better adherence to recommendations (with 34%, 30%, and 18% of inappropriate requests, respectively). Only 4.9% of patients underwent comprehensive aPL testing per international standards (Sidney criteria). Among the 115 aPL-positive cases, multiple antibody positivity was more common in appropriate test requests. Inappropriate requests often stemmed from conditions without established links to APS, such as alopecia, hypercholesterolemia, and dysmenorrhea. A considerable proportion of aPL testing in routine practice lacks clinical justification, reflecting variability in guideline adherence across specialties. Inappropriate testing increases healthcare costs, specialist referrals, and environmental burdens. Improved education, adherence to diagnostic recommendations, and sustainable practices are critical to optimizing APS testing and resource utilization.
期刊介绍:
IMMUNOLOGIC RESEARCH represents a unique medium for the presentation, interpretation, and clarification of complex scientific data. Information is presented in the form of interpretive synthesis reviews, original research articles, symposia, editorials, and theoretical essays. The scope of coverage extends to cellular immunology, immunogenetics, molecular and structural immunology, immunoregulation and autoimmunity, immunopathology, tumor immunology, host defense and microbial immunity, including viral immunology, immunohematology, mucosal immunity, complement, transplantation immunology, clinical immunology, neuroimmunology, immunoendocrinology, immunotoxicology, translational immunology, and history of immunology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


