Katherine L Olivares, Arun Sherma, Chiu Yuen To, Syeda Maria Muzammil
{"title":"头皮切开加半脑部分切除术治疗恶性大脑中动脉梗死:一例说明性病例。","authors":"Katherine L Olivares, Arun Sherma, Chiu Yuen To, Syeda Maria Muzammil","doi":"10.3171/CASE2523","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Malignant middle cerebral artery (MCA) infarctions result in cerebral edema that can lead to brain herniation and death. Standard management includes decompressive hemicraniectomy (DHC) and comprehensive neurocritical care. Some patients may continue to decline despite these measures. Reopening of the scalp incision may allow for additional decompression and provide mortality benefit.</p><p><strong>Observations: </strong>A 47-year-old man developed malignant right MCA territory infarction following intravenous thrombolysis and unsuccessful mechanical thrombectomy. Despite aggressive hyperosmolar therapy and a large DHC, the patient continued to exhibit clinical decline and radiological progression of cerebral edema. In response, the scalp incision was reopened to facilitate maximal external cerebral herniation, a strategy the authors believe was critical in managing the brain swelling. The patient was maintained on prophylactic antibiotics during this period, given the increased infection risk associated with exposed brain surface and potential CSF leakage. Following the resolution of cerebral swelling, a right partial hemispherectomy was performed to excise the infarcted hemisphere. Notably, the patient achieved significant functional recovery following the intervention and an extended period of rehabilitation.</p><p><strong>Lessons: </strong>This case highlights the complexities encountered in the surgical management of malignant cerebral infarction, particularly when standard decompressive measures fail. https://thejns.org/doi/10.3171/CASE2523.</p>","PeriodicalId":94098,"journal":{"name":"Journal of neurosurgery. Case lessons","volume":"10 11","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-09-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435381/pdf/","citationCount":"0","resultStr":"{\"title\":\"Managing malignant middle cerebral artery infarction with open scalp incision and partial hemispherectomy: illustrative case.\",\"authors\":\"Katherine L Olivares, Arun Sherma, Chiu Yuen To, Syeda Maria Muzammil\",\"doi\":\"10.3171/CASE2523\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Malignant middle cerebral artery (MCA) infarctions result in cerebral edema that can lead to brain herniation and death. Standard management includes decompressive hemicraniectomy (DHC) and comprehensive neurocritical care. Some patients may continue to decline despite these measures. Reopening of the scalp incision may allow for additional decompression and provide mortality benefit.</p><p><strong>Observations: </strong>A 47-year-old man developed malignant right MCA territory infarction following intravenous thrombolysis and unsuccessful mechanical thrombectomy. Despite aggressive hyperosmolar therapy and a large DHC, the patient continued to exhibit clinical decline and radiological progression of cerebral edema. In response, the scalp incision was reopened to facilitate maximal external cerebral herniation, a strategy the authors believe was critical in managing the brain swelling. The patient was maintained on prophylactic antibiotics during this period, given the increased infection risk associated with exposed brain surface and potential CSF leakage. Following the resolution of cerebral swelling, a right partial hemispherectomy was performed to excise the infarcted hemisphere. Notably, the patient achieved significant functional recovery following the intervention and an extended period of rehabilitation.</p><p><strong>Lessons: </strong>This case highlights the complexities encountered in the surgical management of malignant cerebral infarction, particularly when standard decompressive measures fail. https://thejns.org/doi/10.3171/CASE2523.</p>\",\"PeriodicalId\":94098,\"journal\":{\"name\":\"Journal of neurosurgery. Case lessons\",\"volume\":\"10 11\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12435381/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of neurosurgery. Case lessons\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3171/CASE2523\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of neurosurgery. Case lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE2523","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Managing malignant middle cerebral artery infarction with open scalp incision and partial hemispherectomy: illustrative case.
Background: Malignant middle cerebral artery (MCA) infarctions result in cerebral edema that can lead to brain herniation and death. Standard management includes decompressive hemicraniectomy (DHC) and comprehensive neurocritical care. Some patients may continue to decline despite these measures. Reopening of the scalp incision may allow for additional decompression and provide mortality benefit.
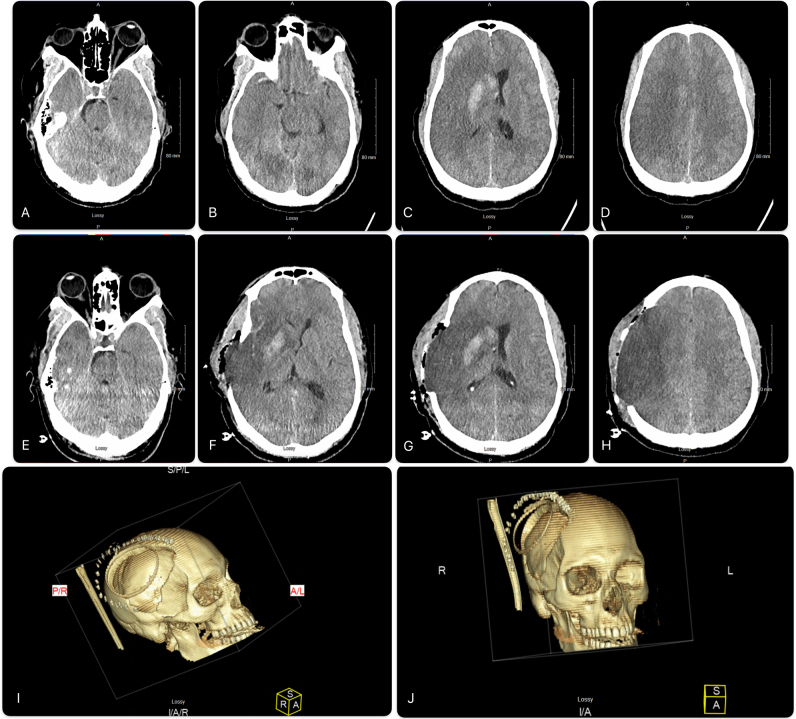
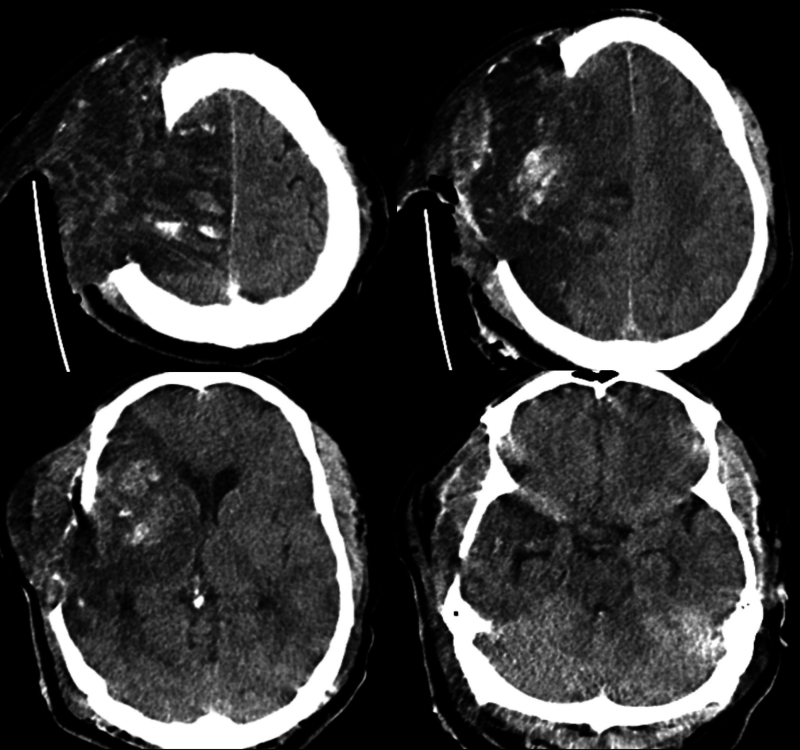
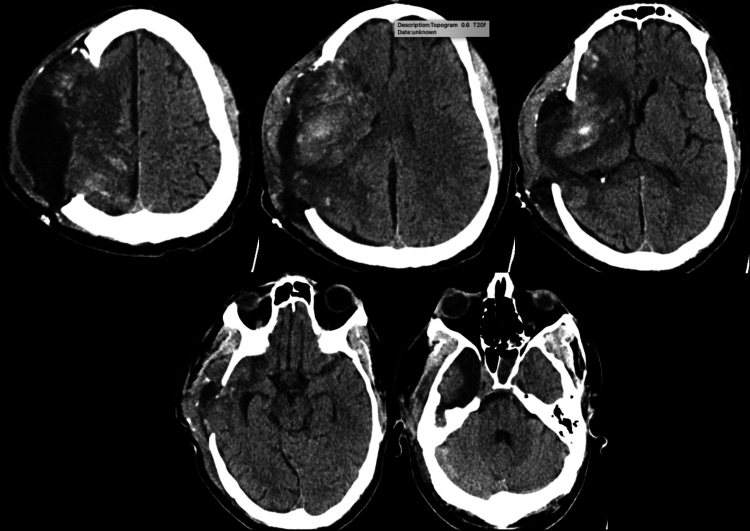
Observations: A 47-year-old man developed malignant right MCA territory infarction following intravenous thrombolysis and unsuccessful mechanical thrombectomy. Despite aggressive hyperosmolar therapy and a large DHC, the patient continued to exhibit clinical decline and radiological progression of cerebral edema. In response, the scalp incision was reopened to facilitate maximal external cerebral herniation, a strategy the authors believe was critical in managing the brain swelling. The patient was maintained on prophylactic antibiotics during this period, given the increased infection risk associated with exposed brain surface and potential CSF leakage. Following the resolution of cerebral swelling, a right partial hemispherectomy was performed to excise the infarcted hemisphere. Notably, the patient achieved significant functional recovery following the intervention and an extended period of rehabilitation.
Lessons: This case highlights the complexities encountered in the surgical management of malignant cerebral infarction, particularly when standard decompressive measures fail. https://thejns.org/doi/10.3171/CASE2523.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


