{"title":"鼻咽癌模拟颅内病变:1例报告及文献复习。","authors":"Ying Zilan, Zhimin Ye","doi":"10.12659/AJCR.947790","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Nasopharyngeal carcinoma can directly invade the intracranial cavity through skull base foramina in advanced-stage patients. Due to both the multiple cranial nerve injuries associated with nasopharyngeal base invasion and the proximity of the pituitary gland, it is challenging to differentiate this condition from intracranial space-occupying lesions, such as meningiomas and pituitary adenomas, in the early stages. This report describes a 37-year-old woman with bilateral nasal congestion, diplopia, hearing loss, and headache diagnosed with a large nasopharyngeal carcinoma invading the cerebellum, pons, medulla oblongata, and cervical spinal cord. CASE REPORT A 37-year-old woman with nasopharyngeal carcinoma (NPC) exhibiting extensive intracranial invasion - involving the mesencephalon, cerebellum, pons, medulla oblongata, and cervical spinal cord - was, with difficulty, diagnosed as having intracranial space-occupying lesions (meningiomas/pituitary tumors) by some renowned neurosurgical centers. She came to our hospital using a wheelchair, exhibiting vague pronunciation, decreased bilateral hearing, headache, facial numbness, diplopia, and coughing when drinking water. Following definitive diagnosis through nasopharyngeal biopsy confirming non-keratinizing carcinoma, we quickly proceeded with treatment. After receiving 6 cycles of chemotherapy with anti-PD-1 immunotherapy, followed by tomotherapy with concurrent nivolumab, the lesion was dynamically reduced, and efficacy was assessed as a complete response (CR). Therapy significantly improved her symptoms, with the holocranial headache resolving, intelligible speech restored, and facial sensation recovered. CONCLUSIONS This case highlights the importance of routinely integrating nasopharyngeal MRI and biopsy when evaluating patients with atypical cranial neuropathies. Furthermore, multidisciplinary team (MDT) collaboration is essential to avoid delayed diagnosis in NPC cases with extensive skull base invasion.</p>","PeriodicalId":39064,"journal":{"name":"American Journal of Case Reports","volume":"26 ","pages":"e947790"},"PeriodicalIF":0.7000,"publicationDate":"2025-09-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449837/pdf/","citationCount":"0","resultStr":"{\"title\":\"Nasopharyngeal Giant Carcinoma Mimicking Intracranial Lesions: A Case Report and Literature Review.\",\"authors\":\"Ying Zilan, Zhimin Ye\",\"doi\":\"10.12659/AJCR.947790\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BACKGROUND Nasopharyngeal carcinoma can directly invade the intracranial cavity through skull base foramina in advanced-stage patients. Due to both the multiple cranial nerve injuries associated with nasopharyngeal base invasion and the proximity of the pituitary gland, it is challenging to differentiate this condition from intracranial space-occupying lesions, such as meningiomas and pituitary adenomas, in the early stages. This report describes a 37-year-old woman with bilateral nasal congestion, diplopia, hearing loss, and headache diagnosed with a large nasopharyngeal carcinoma invading the cerebellum, pons, medulla oblongata, and cervical spinal cord. CASE REPORT A 37-year-old woman with nasopharyngeal carcinoma (NPC) exhibiting extensive intracranial invasion - involving the mesencephalon, cerebellum, pons, medulla oblongata, and cervical spinal cord - was, with difficulty, diagnosed as having intracranial space-occupying lesions (meningiomas/pituitary tumors) by some renowned neurosurgical centers. She came to our hospital using a wheelchair, exhibiting vague pronunciation, decreased bilateral hearing, headache, facial numbness, diplopia, and coughing when drinking water. Following definitive diagnosis through nasopharyngeal biopsy confirming non-keratinizing carcinoma, we quickly proceeded with treatment. After receiving 6 cycles of chemotherapy with anti-PD-1 immunotherapy, followed by tomotherapy with concurrent nivolumab, the lesion was dynamically reduced, and efficacy was assessed as a complete response (CR). Therapy significantly improved her symptoms, with the holocranial headache resolving, intelligible speech restored, and facial sensation recovered. CONCLUSIONS This case highlights the importance of routinely integrating nasopharyngeal MRI and biopsy when evaluating patients with atypical cranial neuropathies. Furthermore, multidisciplinary team (MDT) collaboration is essential to avoid delayed diagnosis in NPC cases with extensive skull base invasion.</p>\",\"PeriodicalId\":39064,\"journal\":{\"name\":\"American Journal of Case Reports\",\"volume\":\"26 \",\"pages\":\"e947790\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-09-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12449837/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12659/AJCR.947790\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.947790","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Nasopharyngeal Giant Carcinoma Mimicking Intracranial Lesions: A Case Report and Literature Review.
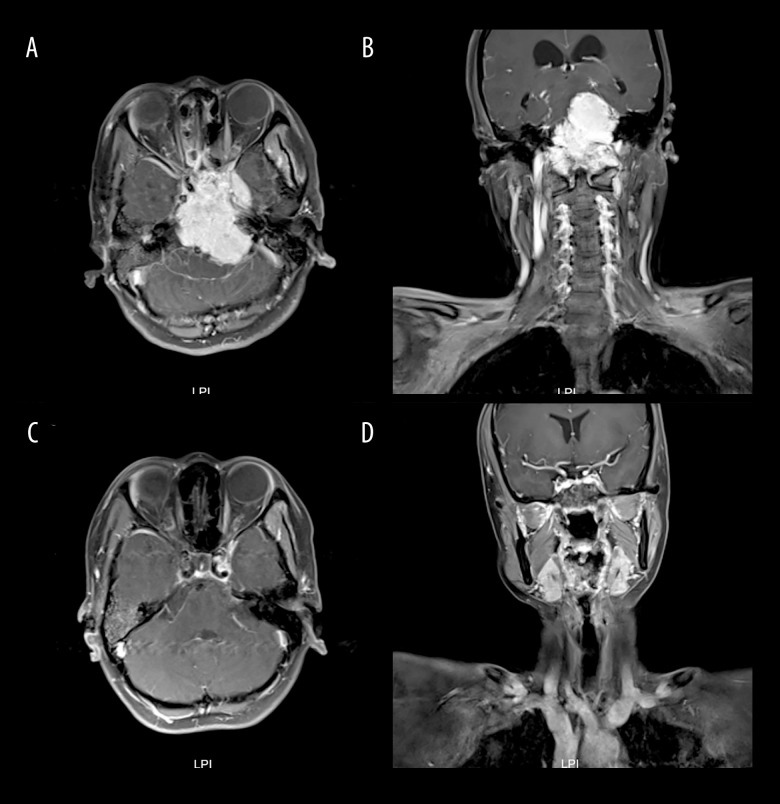
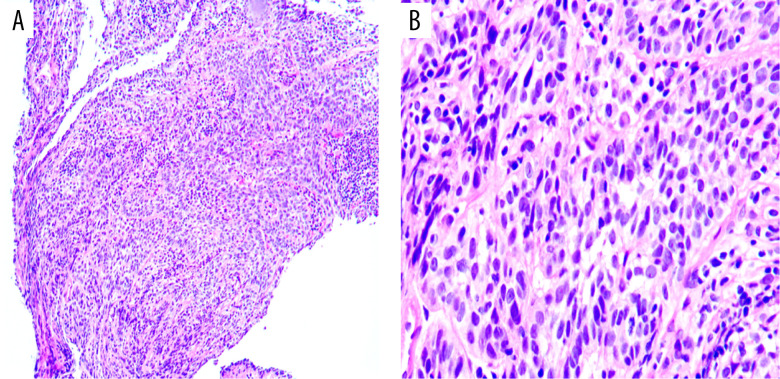
BACKGROUND Nasopharyngeal carcinoma can directly invade the intracranial cavity through skull base foramina in advanced-stage patients. Due to both the multiple cranial nerve injuries associated with nasopharyngeal base invasion and the proximity of the pituitary gland, it is challenging to differentiate this condition from intracranial space-occupying lesions, such as meningiomas and pituitary adenomas, in the early stages. This report describes a 37-year-old woman with bilateral nasal congestion, diplopia, hearing loss, and headache diagnosed with a large nasopharyngeal carcinoma invading the cerebellum, pons, medulla oblongata, and cervical spinal cord. CASE REPORT A 37-year-old woman with nasopharyngeal carcinoma (NPC) exhibiting extensive intracranial invasion - involving the mesencephalon, cerebellum, pons, medulla oblongata, and cervical spinal cord - was, with difficulty, diagnosed as having intracranial space-occupying lesions (meningiomas/pituitary tumors) by some renowned neurosurgical centers. She came to our hospital using a wheelchair, exhibiting vague pronunciation, decreased bilateral hearing, headache, facial numbness, diplopia, and coughing when drinking water. Following definitive diagnosis through nasopharyngeal biopsy confirming non-keratinizing carcinoma, we quickly proceeded with treatment. After receiving 6 cycles of chemotherapy with anti-PD-1 immunotherapy, followed by tomotherapy with concurrent nivolumab, the lesion was dynamically reduced, and efficacy was assessed as a complete response (CR). Therapy significantly improved her symptoms, with the holocranial headache resolving, intelligible speech restored, and facial sensation recovered. CONCLUSIONS This case highlights the importance of routinely integrating nasopharyngeal MRI and biopsy when evaluating patients with atypical cranial neuropathies. Furthermore, multidisciplinary team (MDT) collaboration is essential to avoid delayed diagnosis in NPC cases with extensive skull base invasion.
期刊介绍:
American Journal of Case Reports is an international, peer-reviewed scientific journal that publishes single and series case reports in all medical fields. American Journal of Case Reports is issued on a continuous basis as a primary electronic journal. Print copies of a single article or a set of articles can be ordered on demand.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


