{"title":"β-内酰胺辅助治疗与万古霉素或达托霉素单药治疗耐甲氧西林金黄色葡萄球菌血症的成人患者的比较:最新的系统评价、荟萃分析和试验序列分析","authors":"Changyun Zhao, Wenchao Mao, Difan Lu, Kailun Cai, Changqin Chen, Weihang Hu, Shanmei Lv, Qi Yang","doi":"10.1155/cjid/3972494","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> This study evaluated the efficacy and safety of vancomycin (VAN) or daptomycin (DAP) combined with β-lactams (BLs) versus monotherapy (STAN) for <i>methicillin-resistant Staphylococcus aureus</i> (MRSA) bacteremia. <b>Methods:</b> PubMed, Web of Science, Embase, and Cochrane Library were searched until September 30, 2024, for RCTs or cohort studies comparing combination therapy (COMBO) and STAN in adult MRSA bacteremia. Outcomes included all-cause mortality, 30-day mortality, clinical failure, and safety. Subgroup and trial sequential analyses were performed. <b>Results:</b> Among 22 studies (3214 patients), the COMBO group did not reduce all-cause mortality (RR = 1.16, 95% CI: 0.91-1.48, <i>p</i>=0.24) and 30-day mortality (RR = 1.18, 95% CI: 0.86-1.62, <i>p</i>=0.31). Subgroup analyses suggested increased all-cause mortality in high-quality studies (RR = 1.29, 95% CI: 1.00-1.67, <i>p</i>=0.05). Additionally, when VAN/DAP was administered randomly, COMBO was associated with higher all-cause mortality (RR = 1.37, 95% CI: 1.05-1.78, <i>p</i>=0.02) and 30-day mortality (RR = 1.41, 95% CI: 1.01-1.96, <i>p</i>=0.02). However, the COMBO reduced clinical failure rate (RR = 0.78, 95% CI: 0.65-0.93, <i>p</i>=0.006), persistent bacteremia (RR = 0.70, 95% CI: 0.54-0.92, <i>p</i>=0.01), and relapsed bacteremia (RR = 0.62, 95% CI: 0.48-0.80, <i>p</i>=0.0003). No differences were observed in the microbiological failure rate, duration of bacteremia, or length of hospital stay. Furthermore, the COMBO group showed no significant increase in the incidence of acute kidney injury (AKI). <b>Conclusions:</b> COMBO did not lower mortality in MRSA bacteremia and may increase risk in certain subgroups. However, it improved microbiological outcomes without raising AKI risk. However, these microbiological advantages must be weighed against two concerning findings: a nonsignificant trend toward increased Clostridium difficile infection (CDI) risk and elevated mortality signals in high-quality subgroup analyses. Given conflicting mortality signals, cautious clinical application and further RCTs are needed.</p>","PeriodicalId":50715,"journal":{"name":"Canadian Journal of Infectious Diseases & Medical Microbiology","volume":"2025 ","pages":"3972494"},"PeriodicalIF":2.6000,"publicationDate":"2025-09-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425631/pdf/","citationCount":"0","resultStr":"{\"title\":\"β-Lactam Adjunctive Therapy Compared to Vancomycin or Daptomycin Monotherapy in Adult Patients With Methicillin-Resistant <i>Staphylococcus aureus</i> Bacteremia: An Update Systematic Review, Meta-Analysis, and Trial Sequential Analysis.\",\"authors\":\"Changyun Zhao, Wenchao Mao, Difan Lu, Kailun Cai, Changqin Chen, Weihang Hu, Shanmei Lv, Qi Yang\",\"doi\":\"10.1155/cjid/3972494\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background:</b> This study evaluated the efficacy and safety of vancomycin (VAN) or daptomycin (DAP) combined with β-lactams (BLs) versus monotherapy (STAN) for <i>methicillin-resistant Staphylococcus aureus</i> (MRSA) bacteremia. <b>Methods:</b> PubMed, Web of Science, Embase, and Cochrane Library were searched until September 30, 2024, for RCTs or cohort studies comparing combination therapy (COMBO) and STAN in adult MRSA bacteremia. Outcomes included all-cause mortality, 30-day mortality, clinical failure, and safety. Subgroup and trial sequential analyses were performed. <b>Results:</b> Among 22 studies (3214 patients), the COMBO group did not reduce all-cause mortality (RR = 1.16, 95% CI: 0.91-1.48, <i>p</i>=0.24) and 30-day mortality (RR = 1.18, 95% CI: 0.86-1.62, <i>p</i>=0.31). Subgroup analyses suggested increased all-cause mortality in high-quality studies (RR = 1.29, 95% CI: 1.00-1.67, <i>p</i>=0.05). Additionally, when VAN/DAP was administered randomly, COMBO was associated with higher all-cause mortality (RR = 1.37, 95% CI: 1.05-1.78, <i>p</i>=0.02) and 30-day mortality (RR = 1.41, 95% CI: 1.01-1.96, <i>p</i>=0.02). However, the COMBO reduced clinical failure rate (RR = 0.78, 95% CI: 0.65-0.93, <i>p</i>=0.006), persistent bacteremia (RR = 0.70, 95% CI: 0.54-0.92, <i>p</i>=0.01), and relapsed bacteremia (RR = 0.62, 95% CI: 0.48-0.80, <i>p</i>=0.0003). No differences were observed in the microbiological failure rate, duration of bacteremia, or length of hospital stay. Furthermore, the COMBO group showed no significant increase in the incidence of acute kidney injury (AKI). <b>Conclusions:</b> COMBO did not lower mortality in MRSA bacteremia and may increase risk in certain subgroups. However, it improved microbiological outcomes without raising AKI risk. However, these microbiological advantages must be weighed against two concerning findings: a nonsignificant trend toward increased Clostridium difficile infection (CDI) risk and elevated mortality signals in high-quality subgroup analyses. Given conflicting mortality signals, cautious clinical application and further RCTs are needed.</p>\",\"PeriodicalId\":50715,\"journal\":{\"name\":\"Canadian Journal of Infectious Diseases & Medical Microbiology\",\"volume\":\"2025 \",\"pages\":\"3972494\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-09-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425631/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Infectious Diseases & Medical Microbiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1155/cjid/3972494\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"INFECTIOUS DISEASES\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Infectious Diseases & Medical Microbiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1155/cjid/3972494","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"INFECTIOUS DISEASES","Score":null,"Total":0}
β-Lactam Adjunctive Therapy Compared to Vancomycin or Daptomycin Monotherapy in Adult Patients With Methicillin-Resistant Staphylococcus aureus Bacteremia: An Update Systematic Review, Meta-Analysis, and Trial Sequential Analysis.
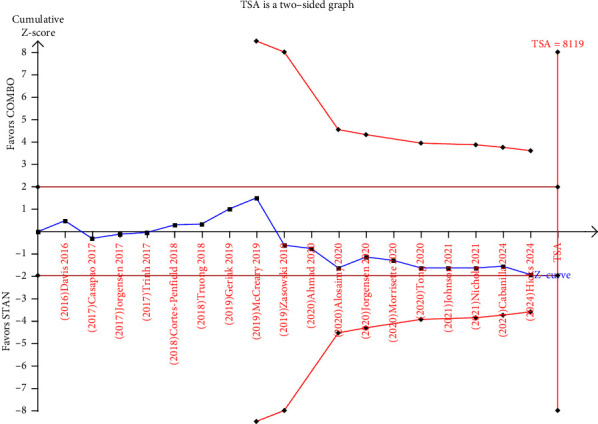
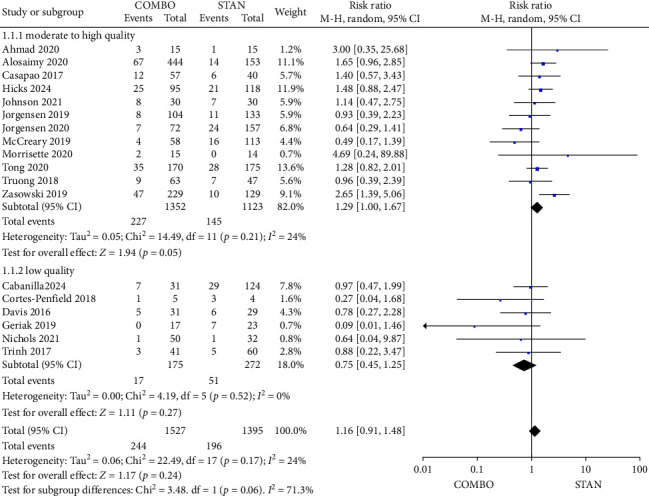
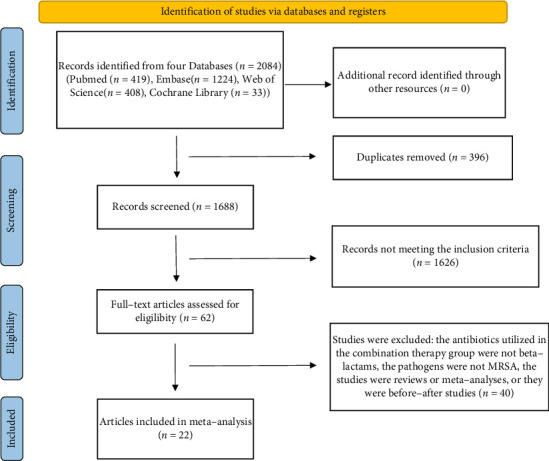
Background: This study evaluated the efficacy and safety of vancomycin (VAN) or daptomycin (DAP) combined with β-lactams (BLs) versus monotherapy (STAN) for methicillin-resistant Staphylococcus aureus (MRSA) bacteremia. Methods: PubMed, Web of Science, Embase, and Cochrane Library were searched until September 30, 2024, for RCTs or cohort studies comparing combination therapy (COMBO) and STAN in adult MRSA bacteremia. Outcomes included all-cause mortality, 30-day mortality, clinical failure, and safety. Subgroup and trial sequential analyses were performed. Results: Among 22 studies (3214 patients), the COMBO group did not reduce all-cause mortality (RR = 1.16, 95% CI: 0.91-1.48, p=0.24) and 30-day mortality (RR = 1.18, 95% CI: 0.86-1.62, p=0.31). Subgroup analyses suggested increased all-cause mortality in high-quality studies (RR = 1.29, 95% CI: 1.00-1.67, p=0.05). Additionally, when VAN/DAP was administered randomly, COMBO was associated with higher all-cause mortality (RR = 1.37, 95% CI: 1.05-1.78, p=0.02) and 30-day mortality (RR = 1.41, 95% CI: 1.01-1.96, p=0.02). However, the COMBO reduced clinical failure rate (RR = 0.78, 95% CI: 0.65-0.93, p=0.006), persistent bacteremia (RR = 0.70, 95% CI: 0.54-0.92, p=0.01), and relapsed bacteremia (RR = 0.62, 95% CI: 0.48-0.80, p=0.0003). No differences were observed in the microbiological failure rate, duration of bacteremia, or length of hospital stay. Furthermore, the COMBO group showed no significant increase in the incidence of acute kidney injury (AKI). Conclusions: COMBO did not lower mortality in MRSA bacteremia and may increase risk in certain subgroups. However, it improved microbiological outcomes without raising AKI risk. However, these microbiological advantages must be weighed against two concerning findings: a nonsignificant trend toward increased Clostridium difficile infection (CDI) risk and elevated mortality signals in high-quality subgroup analyses. Given conflicting mortality signals, cautious clinical application and further RCTs are needed.
期刊介绍:
Canadian Journal of Infectious Diseases and Medical Microbiology is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies related to infectious diseases of bacterial, viral and parasitic origin. The journal welcomes articles describing research on pathogenesis, epidemiology of infection, diagnosis and treatment, antibiotics and resistance, and immunology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


