Jie Zheng, Wei-Kang Ye, Jin Wang, Yi-Nong Zhou, Ting-Ting Yu
{"title":"术前白细胞介素-17a作为胰十二指肠切除术后急性胰腺炎的预测因子。","authors":"Jie Zheng, Wei-Kang Ye, Jin Wang, Yi-Nong Zhou, Ting-Ting Yu","doi":"10.4240/wjgs.v17.i8.105112","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute pancreatitis (AP) is a potentially life-threatening complication of pancreaticoduodenectomy that increases morbidity and mortality in patients. Interleukin-17A (IL-17a) the potential preoperative marker for predicting postoperative outcomes. The purpose of this study is to retrospectively assess the prognostic value of preoperative IL-17a level in prediction of AP and related postoperative pancreatic fistula (POPF) following pancreaticoduodenectomy.</p><p><strong>Aim: </strong>To retrospectively assess the prognostic value of preoperative IL-17a levels in predicting AP and related POPF following pancreaticoduodenectomy.</p><p><strong>Methods: </strong>Retrospective analysis of pancreaticoduodenectomies performed on patients 150 patients between 2017 and 2023. Clinical data including pre-operative IL-17a levels were collected. The primary composite outcomes were postoperative AP and postoperative pancreatic (PP), and the predictive performances of IL-17a levels and fluid load status for postoperative complications were evaluated by statistical analysis.</p><p><strong>Results: </strong>A total of 150 patients were included, and 26 patients (17.3%) developed postoperative AP and 34 patients (22.7%) developed PP. Preoperative IL-17a was a risk factor for postoperative AP (<i>P</i> = 0.03). Furthermore, excessive intraoperative fluid load was a significantly associated (<i>P</i> = 0.01) with PP. The model (IL-17a levels + fluid load status) was highly accurate.</p><p><strong>Conclusion: </strong>Preoperative IL-17a levels and intravascular volume status may serve as useful predictors of AP and subsequent PP following PD. These parameters provide means to evaluate preoperative risk and may guide clinical decision making to enhance postoperative recovery.</p>","PeriodicalId":23759,"journal":{"name":"World Journal of Gastrointestinal Surgery","volume":"17 8","pages":"105112"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12427066/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preoperative interleukin-17a as a predictor of acute pancreatitis after pancreaticoduodenectomy.\",\"authors\":\"Jie Zheng, Wei-Kang Ye, Jin Wang, Yi-Nong Zhou, Ting-Ting Yu\",\"doi\":\"10.4240/wjgs.v17.i8.105112\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute pancreatitis (AP) is a potentially life-threatening complication of pancreaticoduodenectomy that increases morbidity and mortality in patients. Interleukin-17A (IL-17a) the potential preoperative marker for predicting postoperative outcomes. The purpose of this study is to retrospectively assess the prognostic value of preoperative IL-17a level in prediction of AP and related postoperative pancreatic fistula (POPF) following pancreaticoduodenectomy.</p><p><strong>Aim: </strong>To retrospectively assess the prognostic value of preoperative IL-17a levels in predicting AP and related POPF following pancreaticoduodenectomy.</p><p><strong>Methods: </strong>Retrospective analysis of pancreaticoduodenectomies performed on patients 150 patients between 2017 and 2023. Clinical data including pre-operative IL-17a levels were collected. The primary composite outcomes were postoperative AP and postoperative pancreatic (PP), and the predictive performances of IL-17a levels and fluid load status for postoperative complications were evaluated by statistical analysis.</p><p><strong>Results: </strong>A total of 150 patients were included, and 26 patients (17.3%) developed postoperative AP and 34 patients (22.7%) developed PP. Preoperative IL-17a was a risk factor for postoperative AP (<i>P</i> = 0.03). Furthermore, excessive intraoperative fluid load was a significantly associated (<i>P</i> = 0.01) with PP. The model (IL-17a levels + fluid load status) was highly accurate.</p><p><strong>Conclusion: </strong>Preoperative IL-17a levels and intravascular volume status may serve as useful predictors of AP and subsequent PP following PD. These parameters provide means to evaluate preoperative risk and may guide clinical decision making to enhance postoperative recovery.</p>\",\"PeriodicalId\":23759,\"journal\":{\"name\":\"World Journal of Gastrointestinal Surgery\",\"volume\":\"17 8\",\"pages\":\"105112\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12427066/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4240/wjgs.v17.i8.105112\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4240/wjgs.v17.i8.105112","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Preoperative interleukin-17a as a predictor of acute pancreatitis after pancreaticoduodenectomy.
Background: Acute pancreatitis (AP) is a potentially life-threatening complication of pancreaticoduodenectomy that increases morbidity and mortality in patients. Interleukin-17A (IL-17a) the potential preoperative marker for predicting postoperative outcomes. The purpose of this study is to retrospectively assess the prognostic value of preoperative IL-17a level in prediction of AP and related postoperative pancreatic fistula (POPF) following pancreaticoduodenectomy.
Aim: To retrospectively assess the prognostic value of preoperative IL-17a levels in predicting AP and related POPF following pancreaticoduodenectomy.
Methods: Retrospective analysis of pancreaticoduodenectomies performed on patients 150 patients between 2017 and 2023. Clinical data including pre-operative IL-17a levels were collected. The primary composite outcomes were postoperative AP and postoperative pancreatic (PP), and the predictive performances of IL-17a levels and fluid load status for postoperative complications were evaluated by statistical analysis.
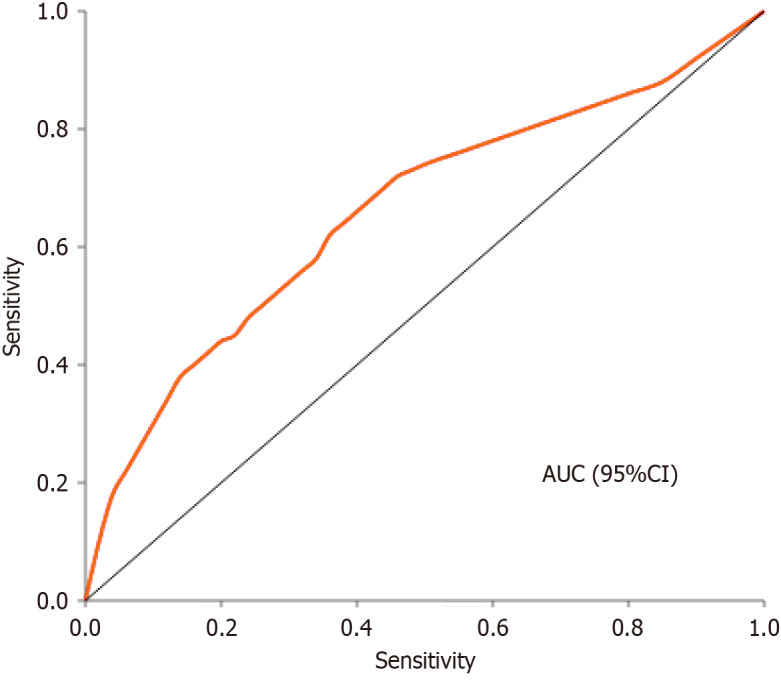
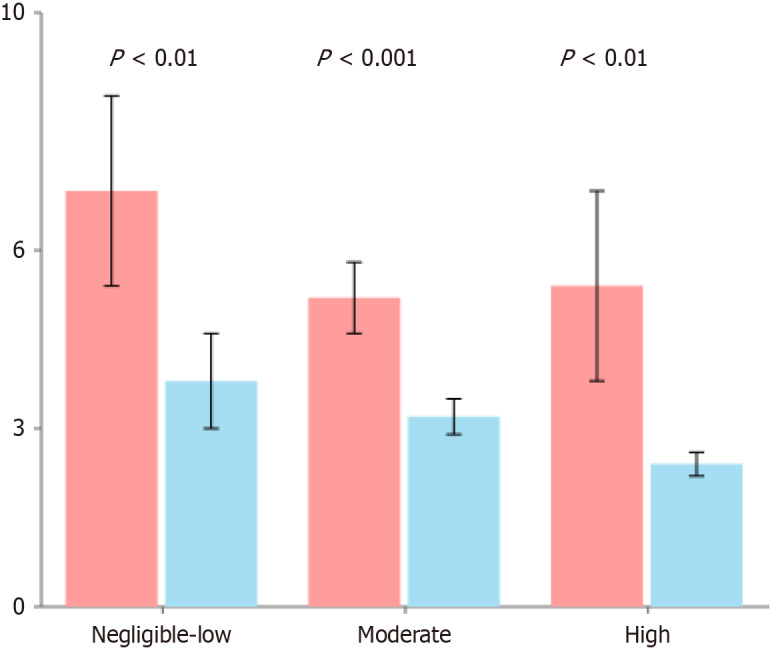
Results: A total of 150 patients were included, and 26 patients (17.3%) developed postoperative AP and 34 patients (22.7%) developed PP. Preoperative IL-17a was a risk factor for postoperative AP (P = 0.03). Furthermore, excessive intraoperative fluid load was a significantly associated (P = 0.01) with PP. The model (IL-17a levels + fluid load status) was highly accurate.
Conclusion: Preoperative IL-17a levels and intravascular volume status may serve as useful predictors of AP and subsequent PP following PD. These parameters provide means to evaluate preoperative risk and may guide clinical decision making to enhance postoperative recovery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


