{"title":"以呕吐和心力衰竭为表现的嗜铬细胞瘤1例。","authors":"Han Cheng, Ling-Tong Gu, Jing Yang","doi":"10.4330/wjc.v17.i8.110366","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pheochromocytoma, a rare catecholamine-secreting tumor, typically presents with the classic triad of headache, palpitations, and diaphoresis, often accompanied by cardiovascular manifestations. While vomiting occurs in approximately 34.5% of cases, it is rarely the predominant and persistent presenting symptom. Pheochromocytoma-induced cardiomyopathy leading to heart failure is a recognized but uncommon complication. Due to its heterogeneous presentations, misdiagnosis and diagnostic delay are frequent.</p><p><strong>Case summary: </strong>A 53-year-old female presented predominantly with persistent and refractory vomiting as her chief complaint, accompanied by signs of acute heart failure [left ventricular ejection fraction (LVEF) 30%]. Initial evaluation at a primary hospital, including coronary angiography (revealing only mild stenosis), led to a misdiagnosis of coronary artery disease. Despite standard anti-thrombotic, anti-heart failure, and anti-emetic therapy, her vomiting persisted and heart failure did not resolve. Subsequent hospitalization revealed dramatic paroxysmal hypertension (202/129 mmHg to 97/51 mmHg) and fever. Significantly elevated plasma metanephrines and normetanephrine, combined with abdominal computed tomography and magnetic resonance imaging, confirmed a right adrenal pheochromocytoma. This diagnosis was significantly delayed due to the atypical prominence of gastrointestinal symptoms masking the underlying endocrine crisis.</p><p><strong>Conclusion: </strong>This case highlights a highly atypical presentation of pheochromocytoma dominated by refractory vomiting and complicated by acute catecholamine-induced cardiomyopathy. It emphatically underscores that pheochromocytoma must be considered in the differential diagnosis for patients presenting with unexplained, treatment-resistant vomiting, particularly when co-existing with acute heart failure. The presence of labile hypertension, even if not initially evident, provides a crucial diagnostic clue. Prompt biochemical screening (catecholamine metabolites) and adrenal imaging are essential to prevent diagnostic delay and enable timely, life-saving surgical intervention.</p>","PeriodicalId":23800,"journal":{"name":"World Journal of Cardiology","volume":"17 8","pages":"110366"},"PeriodicalIF":2.8000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12427064/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pheochromocytoma presenting with vomiting and heart failure: A case report.\",\"authors\":\"Han Cheng, Ling-Tong Gu, Jing Yang\",\"doi\":\"10.4330/wjc.v17.i8.110366\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Pheochromocytoma, a rare catecholamine-secreting tumor, typically presents with the classic triad of headache, palpitations, and diaphoresis, often accompanied by cardiovascular manifestations. While vomiting occurs in approximately 34.5% of cases, it is rarely the predominant and persistent presenting symptom. Pheochromocytoma-induced cardiomyopathy leading to heart failure is a recognized but uncommon complication. Due to its heterogeneous presentations, misdiagnosis and diagnostic delay are frequent.</p><p><strong>Case summary: </strong>A 53-year-old female presented predominantly with persistent and refractory vomiting as her chief complaint, accompanied by signs of acute heart failure [left ventricular ejection fraction (LVEF) 30%]. Initial evaluation at a primary hospital, including coronary angiography (revealing only mild stenosis), led to a misdiagnosis of coronary artery disease. Despite standard anti-thrombotic, anti-heart failure, and anti-emetic therapy, her vomiting persisted and heart failure did not resolve. Subsequent hospitalization revealed dramatic paroxysmal hypertension (202/129 mmHg to 97/51 mmHg) and fever. Significantly elevated plasma metanephrines and normetanephrine, combined with abdominal computed tomography and magnetic resonance imaging, confirmed a right adrenal pheochromocytoma. This diagnosis was significantly delayed due to the atypical prominence of gastrointestinal symptoms masking the underlying endocrine crisis.</p><p><strong>Conclusion: </strong>This case highlights a highly atypical presentation of pheochromocytoma dominated by refractory vomiting and complicated by acute catecholamine-induced cardiomyopathy. It emphatically underscores that pheochromocytoma must be considered in the differential diagnosis for patients presenting with unexplained, treatment-resistant vomiting, particularly when co-existing with acute heart failure. The presence of labile hypertension, even if not initially evident, provides a crucial diagnostic clue. Prompt biochemical screening (catecholamine metabolites) and adrenal imaging are essential to prevent diagnostic delay and enable timely, life-saving surgical intervention.</p>\",\"PeriodicalId\":23800,\"journal\":{\"name\":\"World Journal of Cardiology\",\"volume\":\"17 8\",\"pages\":\"110366\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2025-08-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12427064/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Cardiology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4330/wjc.v17.i8.110366\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Cardiology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4330/wjc.v17.i8.110366","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Pheochromocytoma presenting with vomiting and heart failure: A case report.
Background: Pheochromocytoma, a rare catecholamine-secreting tumor, typically presents with the classic triad of headache, palpitations, and diaphoresis, often accompanied by cardiovascular manifestations. While vomiting occurs in approximately 34.5% of cases, it is rarely the predominant and persistent presenting symptom. Pheochromocytoma-induced cardiomyopathy leading to heart failure is a recognized but uncommon complication. Due to its heterogeneous presentations, misdiagnosis and diagnostic delay are frequent.
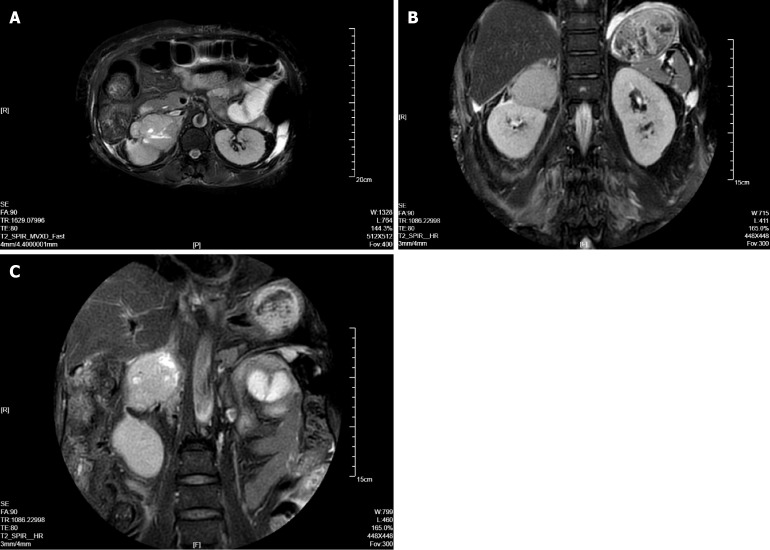
Case summary: A 53-year-old female presented predominantly with persistent and refractory vomiting as her chief complaint, accompanied by signs of acute heart failure [left ventricular ejection fraction (LVEF) 30%]. Initial evaluation at a primary hospital, including coronary angiography (revealing only mild stenosis), led to a misdiagnosis of coronary artery disease. Despite standard anti-thrombotic, anti-heart failure, and anti-emetic therapy, her vomiting persisted and heart failure did not resolve. Subsequent hospitalization revealed dramatic paroxysmal hypertension (202/129 mmHg to 97/51 mmHg) and fever. Significantly elevated plasma metanephrines and normetanephrine, combined with abdominal computed tomography and magnetic resonance imaging, confirmed a right adrenal pheochromocytoma. This diagnosis was significantly delayed due to the atypical prominence of gastrointestinal symptoms masking the underlying endocrine crisis.
Conclusion: This case highlights a highly atypical presentation of pheochromocytoma dominated by refractory vomiting and complicated by acute catecholamine-induced cardiomyopathy. It emphatically underscores that pheochromocytoma must be considered in the differential diagnosis for patients presenting with unexplained, treatment-resistant vomiting, particularly when co-existing with acute heart failure. The presence of labile hypertension, even if not initially evident, provides a crucial diagnostic clue. Prompt biochemical screening (catecholamine metabolites) and adrenal imaging are essential to prevent diagnostic delay and enable timely, life-saving surgical intervention.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


