{"title":"心脏装置的潘多拉盒子:一例卵圆孔闭合后感染性心内膜炎。","authors":"Fulvio Cacciapuoti, Fabio Minicucci, Brenno Fiorani, Ilaria Caso, Mafalda Esposito, Luca Gaetano Tarquinio, Giacomo Mattiello, Elisa Di Pietro, Teresa Russo, Ciro Mauro","doi":"10.4103/jcecho.jcecho_11_25","DOIUrl":null,"url":null,"abstract":"<p><p>Patent foramen ovale (PFO) is a congenital cardiac defect present in approximately 30% of the general population. While often asymptomatic, it is associated with cryptogenic stroke and paradoxical embolism. Percutaneous closure using atrial septal defect occluder is an effective preventive strategy, but these devices carry a risk of rare complications, including infective endocarditis. Device-associated infective endocarditis is often linked to transient bacteremia following invasive procedures, highlighting the importance of antibiotic prophylaxis. However, the clinical presentation can be variable, requiring a high index of suspicion and advanced imaging for the diagnosis. We describe the case of a 55-year-old woman with hypertension, obesity, and a history of PFO closure with an Amplatzer occluder, who developed infective endocarditis weeks after a dental procedure. She presented with fever, vomiting, and confusion, initially misdiagnosed with encephalitis. Transesophageal echocardiography revealed large filamentous vegetation on the Amplatzer occluder, causing functional mitral regurgitation. Blood cultures identified <i>Staphylococcus aureus</i> and <i>Streptococcus pneumoniae</i>, confirming a mixed bacterial infection. The patient underwent surgical removal of the infected device and mitral valve repair. Postoperatively, she improved significantly and was discharged with a complete course of antibiotics. This case underscores the need for vigilance in patients with intracardiac devices, particularly following bacteremia-inducing procedures. Early diagnosis using echocardiography and prompt surgical intervention are essential to managing device-related infective endocarditis. While antibiotic prophylaxis may reduce the risk of bacteremia-related infections, the lack of high-quality evidence necessitates further research to guide preventive strategies. Multidisciplinary care and strict adherence to diagnostic and therapeutic protocols remain pivotal to improving patient outcomes.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"35 2","pages":"175-178"},"PeriodicalIF":1.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425280/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Pandora's Box of Cardiac Devices: A Case of Infective Endocarditis Postpatent Foramen Ovale Closure.\",\"authors\":\"Fulvio Cacciapuoti, Fabio Minicucci, Brenno Fiorani, Ilaria Caso, Mafalda Esposito, Luca Gaetano Tarquinio, Giacomo Mattiello, Elisa Di Pietro, Teresa Russo, Ciro Mauro\",\"doi\":\"10.4103/jcecho.jcecho_11_25\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Patent foramen ovale (PFO) is a congenital cardiac defect present in approximately 30% of the general population. While often asymptomatic, it is associated with cryptogenic stroke and paradoxical embolism. Percutaneous closure using atrial septal defect occluder is an effective preventive strategy, but these devices carry a risk of rare complications, including infective endocarditis. Device-associated infective endocarditis is often linked to transient bacteremia following invasive procedures, highlighting the importance of antibiotic prophylaxis. However, the clinical presentation can be variable, requiring a high index of suspicion and advanced imaging for the diagnosis. We describe the case of a 55-year-old woman with hypertension, obesity, and a history of PFO closure with an Amplatzer occluder, who developed infective endocarditis weeks after a dental procedure. She presented with fever, vomiting, and confusion, initially misdiagnosed with encephalitis. Transesophageal echocardiography revealed large filamentous vegetation on the Amplatzer occluder, causing functional mitral regurgitation. Blood cultures identified <i>Staphylococcus aureus</i> and <i>Streptococcus pneumoniae</i>, confirming a mixed bacterial infection. The patient underwent surgical removal of the infected device and mitral valve repair. Postoperatively, she improved significantly and was discharged with a complete course of antibiotics. This case underscores the need for vigilance in patients with intracardiac devices, particularly following bacteremia-inducing procedures. Early diagnosis using echocardiography and prompt surgical intervention are essential to managing device-related infective endocarditis. While antibiotic prophylaxis may reduce the risk of bacteremia-related infections, the lack of high-quality evidence necessitates further research to guide preventive strategies. Multidisciplinary care and strict adherence to diagnostic and therapeutic protocols remain pivotal to improving patient outcomes.</p>\",\"PeriodicalId\":15191,\"journal\":{\"name\":\"Journal of Cardiovascular Echography\",\"volume\":\"35 2\",\"pages\":\"175-178\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425280/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Echography\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jcecho.jcecho_11_25\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_11_25","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The Pandora's Box of Cardiac Devices: A Case of Infective Endocarditis Postpatent Foramen Ovale Closure.
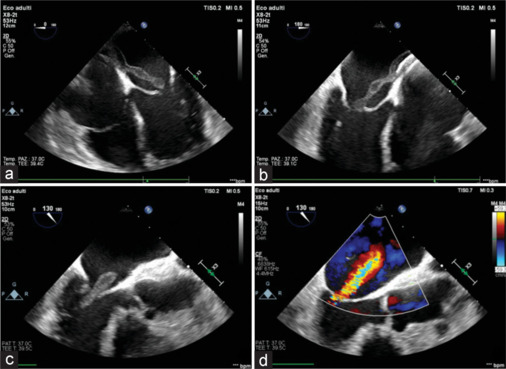
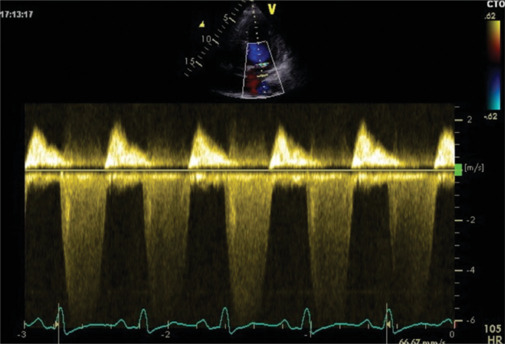
Patent foramen ovale (PFO) is a congenital cardiac defect present in approximately 30% of the general population. While often asymptomatic, it is associated with cryptogenic stroke and paradoxical embolism. Percutaneous closure using atrial septal defect occluder is an effective preventive strategy, but these devices carry a risk of rare complications, including infective endocarditis. Device-associated infective endocarditis is often linked to transient bacteremia following invasive procedures, highlighting the importance of antibiotic prophylaxis. However, the clinical presentation can be variable, requiring a high index of suspicion and advanced imaging for the diagnosis. We describe the case of a 55-year-old woman with hypertension, obesity, and a history of PFO closure with an Amplatzer occluder, who developed infective endocarditis weeks after a dental procedure. She presented with fever, vomiting, and confusion, initially misdiagnosed with encephalitis. Transesophageal echocardiography revealed large filamentous vegetation on the Amplatzer occluder, causing functional mitral regurgitation. Blood cultures identified Staphylococcus aureus and Streptococcus pneumoniae, confirming a mixed bacterial infection. The patient underwent surgical removal of the infected device and mitral valve repair. Postoperatively, she improved significantly and was discharged with a complete course of antibiotics. This case underscores the need for vigilance in patients with intracardiac devices, particularly following bacteremia-inducing procedures. Early diagnosis using echocardiography and prompt surgical intervention are essential to managing device-related infective endocarditis. While antibiotic prophylaxis may reduce the risk of bacteremia-related infections, the lack of high-quality evidence necessitates further research to guide preventive strategies. Multidisciplinary care and strict adherence to diagnostic and therapeutic protocols remain pivotal to improving patient outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


