{"title":"异位冠状动脉栓塞导致腔静脉血栓患者st段抬高型心肌梗死。","authors":"Davide Restelli, Riccardo Molinari, Silvia Massaro, Gianluca Tiberti, Andrea Farina, Scipione Carerj","doi":"10.4103/jcecho.jcecho_75_24","DOIUrl":null,"url":null,"abstract":"<p><p>We present a case of a 48-year-old man with an atypical type 2 myocardial infarction (MI)/myocardial infarction with nonobstructive coronary arteries, caused by a coronary embolism originating from the inferior vena cava and passing through a patent foramen ovale (PFO). The patient presented to the emergency department with oppressive retrosternal chest pain. His medical history included papillary renal cell carcinoma and seminoma with recent abdominal lymph node recurrence. The electrocardiogram indicated an inferolateral ST-segment elevation (STE), prompting emergency coronary angiography, that revealed distal occlusion of the circumflex artery and the obtuse marginal branch, suggesting an embolic etiology. Stent placement was deferred, and the management approach involved thromboaspiration and unfractionated heparin infusion. Abdominal imaging identified a thrombotic formation in the inferior vena cava and a transesophageal echocardiogram revealed a PFO with a right-to-left shunt, supporting the diagnosis of a paradoxical embolism. Follow-up coronary angiography showed vessel patency, and the patient was then treated with low-molecular-weight heparin. This case underscores the importance of considering alternative etiologies for STE myocardial infarction beyond acute plaque rupture, highlighting the need for individualized management strategies, particularly in patients with complex medical histories, and given the lack of standardized treatment guidelines for coronary embolism.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"35 2","pages":"165-168"},"PeriodicalIF":1.0000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425241/pdf/","citationCount":"0","resultStr":"{\"title\":\"Paradoxical Coronary Embolism Leading to ST-segment Elevation Myocardial Infarction in a Patient with Caval Thrombosis.\",\"authors\":\"Davide Restelli, Riccardo Molinari, Silvia Massaro, Gianluca Tiberti, Andrea Farina, Scipione Carerj\",\"doi\":\"10.4103/jcecho.jcecho_75_24\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We present a case of a 48-year-old man with an atypical type 2 myocardial infarction (MI)/myocardial infarction with nonobstructive coronary arteries, caused by a coronary embolism originating from the inferior vena cava and passing through a patent foramen ovale (PFO). The patient presented to the emergency department with oppressive retrosternal chest pain. His medical history included papillary renal cell carcinoma and seminoma with recent abdominal lymph node recurrence. The electrocardiogram indicated an inferolateral ST-segment elevation (STE), prompting emergency coronary angiography, that revealed distal occlusion of the circumflex artery and the obtuse marginal branch, suggesting an embolic etiology. Stent placement was deferred, and the management approach involved thromboaspiration and unfractionated heparin infusion. Abdominal imaging identified a thrombotic formation in the inferior vena cava and a transesophageal echocardiogram revealed a PFO with a right-to-left shunt, supporting the diagnosis of a paradoxical embolism. Follow-up coronary angiography showed vessel patency, and the patient was then treated with low-molecular-weight heparin. This case underscores the importance of considering alternative etiologies for STE myocardial infarction beyond acute plaque rupture, highlighting the need for individualized management strategies, particularly in patients with complex medical histories, and given the lack of standardized treatment guidelines for coronary embolism.</p>\",\"PeriodicalId\":15191,\"journal\":{\"name\":\"Journal of Cardiovascular Echography\",\"volume\":\"35 2\",\"pages\":\"165-168\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2025-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12425241/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular Echography\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jcecho.jcecho_75_24\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/7/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_75_24","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/7/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Paradoxical Coronary Embolism Leading to ST-segment Elevation Myocardial Infarction in a Patient with Caval Thrombosis.
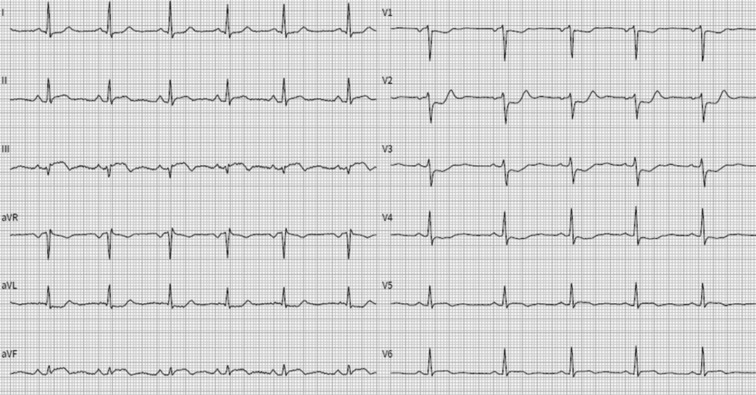
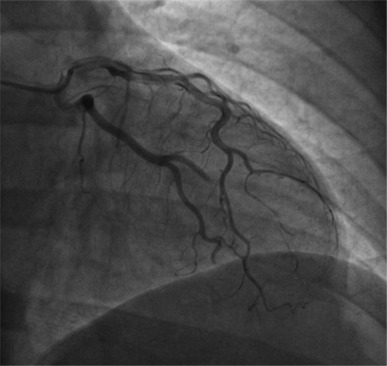
We present a case of a 48-year-old man with an atypical type 2 myocardial infarction (MI)/myocardial infarction with nonobstructive coronary arteries, caused by a coronary embolism originating from the inferior vena cava and passing through a patent foramen ovale (PFO). The patient presented to the emergency department with oppressive retrosternal chest pain. His medical history included papillary renal cell carcinoma and seminoma with recent abdominal lymph node recurrence. The electrocardiogram indicated an inferolateral ST-segment elevation (STE), prompting emergency coronary angiography, that revealed distal occlusion of the circumflex artery and the obtuse marginal branch, suggesting an embolic etiology. Stent placement was deferred, and the management approach involved thromboaspiration and unfractionated heparin infusion. Abdominal imaging identified a thrombotic formation in the inferior vena cava and a transesophageal echocardiogram revealed a PFO with a right-to-left shunt, supporting the diagnosis of a paradoxical embolism. Follow-up coronary angiography showed vessel patency, and the patient was then treated with low-molecular-weight heparin. This case underscores the importance of considering alternative etiologies for STE myocardial infarction beyond acute plaque rupture, highlighting the need for individualized management strategies, particularly in patients with complex medical histories, and given the lack of standardized treatment guidelines for coronary embolism.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


