{"title":"曲妥珠单抗和帕妥珠单抗治疗人表皮生长因子受体2阳性乳腺癌患者的癌症治疗相关心功能障碍","authors":"Reina Ozaki, Ryota Morimoto, Shingo Kazama, Hiroaki Hiraiwa, Toru Kondo, Yuko Takano, Toyone Kikumori, Tomoya Shimokata, Yachiyo Kuwatsuka, Yasuko K Bando, Masahiko Ando, Yuichi Ando, Toyoaki Murohara","doi":"10.1253/circrep.CR-25-0036","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Breast cancer is the most common cancer in women. Although anti-human epidermal growth factor receptor 2 (HER2) therapy is effective in patients with HER2-positive breast cancer, it occasionally induces cancer therapy-related cardiac dysfunction (CTRCD). This study aimed to determine the factors associated with CTRCD in patients with HER2-positive breast cancer treated with trastuzumab.</p><p><strong>Methods and results: </strong>We retrospectively analyzed the data of 286 patients with breast cancer who received trastuzumab. Accordingly, patients were categorized into CTRCD (+) and CTRCD (-) groups to elucidate the factors associated with cardiotoxicity. The median age of patients was 54 years. CTRCD was observed in 13 (4.5%) patients, and 2 (0.7%) patients had severe symptomatic heart failure, with a New York Heart Association class ≥III. All patients with CTRCD had a history of epirubicin use, and patients receiving both trastuzumab and pertuzumab had significantly higher rates of CTRCD (P=0.003); the history of pertuzumab administration was an independent predictor of CTRCD development. The median duration from trastuzumab initiation to CTRCD onset and from CTRCD onset to recovery was 244 (interquartile range [IQR] 164-333) and 122 ([IQR] 38-186) days, respectively.</p><p><strong>Conclusions: </strong>In HER2-positive breast cancer, CTRCD occurred more frequently in patients using anthracycline followed by trastuzumab and pertuzumab simultaneously. Systolic dysfunction was reversible in all patients, and normalization of cardiac function took approximately 4 months from CTRCD onset.</p>","PeriodicalId":94305,"journal":{"name":"Circulation reports","volume":"7 9","pages":"800-808"},"PeriodicalIF":1.1000,"publicationDate":"2025-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12419944/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cancer Therapy-Related Cardiac Dysfunction in Patients With Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer Treated With Trastuzumab and Pertuzumab.\",\"authors\":\"Reina Ozaki, Ryota Morimoto, Shingo Kazama, Hiroaki Hiraiwa, Toru Kondo, Yuko Takano, Toyone Kikumori, Tomoya Shimokata, Yachiyo Kuwatsuka, Yasuko K Bando, Masahiko Ando, Yuichi Ando, Toyoaki Murohara\",\"doi\":\"10.1253/circrep.CR-25-0036\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Breast cancer is the most common cancer in women. Although anti-human epidermal growth factor receptor 2 (HER2) therapy is effective in patients with HER2-positive breast cancer, it occasionally induces cancer therapy-related cardiac dysfunction (CTRCD). This study aimed to determine the factors associated with CTRCD in patients with HER2-positive breast cancer treated with trastuzumab.</p><p><strong>Methods and results: </strong>We retrospectively analyzed the data of 286 patients with breast cancer who received trastuzumab. Accordingly, patients were categorized into CTRCD (+) and CTRCD (-) groups to elucidate the factors associated with cardiotoxicity. The median age of patients was 54 years. CTRCD was observed in 13 (4.5%) patients, and 2 (0.7%) patients had severe symptomatic heart failure, with a New York Heart Association class ≥III. All patients with CTRCD had a history of epirubicin use, and patients receiving both trastuzumab and pertuzumab had significantly higher rates of CTRCD (P=0.003); the history of pertuzumab administration was an independent predictor of CTRCD development. The median duration from trastuzumab initiation to CTRCD onset and from CTRCD onset to recovery was 244 (interquartile range [IQR] 164-333) and 122 ([IQR] 38-186) days, respectively.</p><p><strong>Conclusions: </strong>In HER2-positive breast cancer, CTRCD occurred more frequently in patients using anthracycline followed by trastuzumab and pertuzumab simultaneously. Systolic dysfunction was reversible in all patients, and normalization of cardiac function took approximately 4 months from CTRCD onset.</p>\",\"PeriodicalId\":94305,\"journal\":{\"name\":\"Circulation reports\",\"volume\":\"7 9\",\"pages\":\"800-808\"},\"PeriodicalIF\":1.1000,\"publicationDate\":\"2025-07-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12419944/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Circulation reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1253/circrep.CR-25-0036\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/10 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Circulation reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1253/circrep.CR-25-0036","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/10 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Cancer Therapy-Related Cardiac Dysfunction in Patients With Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer Treated With Trastuzumab and Pertuzumab.
Background: Breast cancer is the most common cancer in women. Although anti-human epidermal growth factor receptor 2 (HER2) therapy is effective in patients with HER2-positive breast cancer, it occasionally induces cancer therapy-related cardiac dysfunction (CTRCD). This study aimed to determine the factors associated with CTRCD in patients with HER2-positive breast cancer treated with trastuzumab.
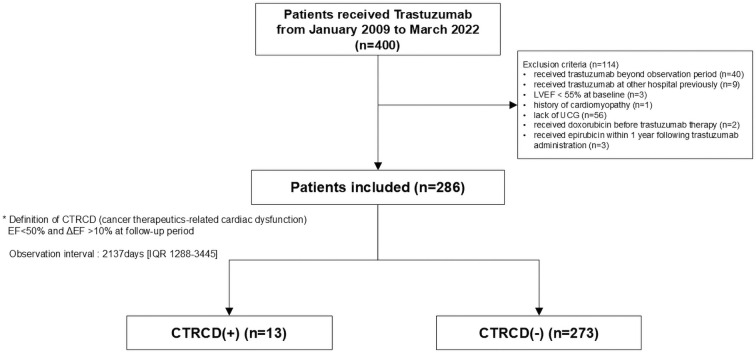
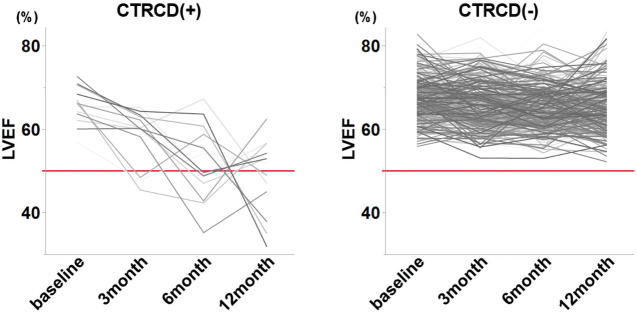
Methods and results: We retrospectively analyzed the data of 286 patients with breast cancer who received trastuzumab. Accordingly, patients were categorized into CTRCD (+) and CTRCD (-) groups to elucidate the factors associated with cardiotoxicity. The median age of patients was 54 years. CTRCD was observed in 13 (4.5%) patients, and 2 (0.7%) patients had severe symptomatic heart failure, with a New York Heart Association class ≥III. All patients with CTRCD had a history of epirubicin use, and patients receiving both trastuzumab and pertuzumab had significantly higher rates of CTRCD (P=0.003); the history of pertuzumab administration was an independent predictor of CTRCD development. The median duration from trastuzumab initiation to CTRCD onset and from CTRCD onset to recovery was 244 (interquartile range [IQR] 164-333) and 122 ([IQR] 38-186) days, respectively.
Conclusions: In HER2-positive breast cancer, CTRCD occurred more frequently in patients using anthracycline followed by trastuzumab and pertuzumab simultaneously. Systolic dysfunction was reversible in all patients, and normalization of cardiac function took approximately 4 months from CTRCD onset.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


