Randy W Lesh, Jino Park, Vincent M Desiato, Martin Matsumura, Thorsen W Haugen
{"title":"气管切开术后围手术期心肌损伤的预测因素及预后。","authors":"Randy W Lesh, Jino Park, Vincent M Desiato, Martin Matsumura, Thorsen W Haugen","doi":"10.1002/wjo2.218","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Perioperative myocardial injury (PMI) is associated with increased mortality. We describe risk factors for and outcomes of PMI in patients undergoing tracheotomy.</p><p><strong>Methods: </strong>Retrospective study of patients undergoing tracheotomy from 2007 to 2016. PMI was defined by a postoperative cardiac troponin I (cTnI) > 99th percentile. Demographics and comorbidities were extracted from the electronic medical record and compared between patients with and without PMI. Significant univariate predictors were included in a multivariable logistic regression model to determine independent predictors of PMI. Thirty-day and 1-year mortality of patients with and without PMI were compared.</p><p><strong>Results: </strong>Of 861 patients undergoing tracheotomy, 41 (4.76%) had PMI and 820 (95.24%) did not. PMI was associated with higher mortality at both 30 days (40.5% vs. 11.2%, <i>p</i> < 0.001) and 1 year (73.2% vs. 44.1%, <i>p</i> < 0.001). Patients with PMI were older (median age 65 vs. 60, <i>p</i> = 0.002) and more likely to have prior myocardial infarction (MI) (36.6% vs. 10.7%, <i>p</i> < 0.001) and chronic kidney disease (31.7% vs. 16.7%, <i>p</i> = 0.024). Cancer diagnosis was associated with a lower risk of PMI (24.4% vs. 41.8%, <i>p</i> = 0.041). Older age (odds ratio [OR] = 1.033, <i>p</i> < 0.001) and prior MI (OR = 3.686, <i>p</i> < 0.001) were independently associated with PMI.</p><p><strong>Conclusion: </strong>Patients with PMI following tracheotomy had increased short- and long-term mortality. Increased age and history of prior MI were independent predictors of PMI, while cancer was associated with a lower risk of PMI following tracheotomy. ICU patients likely have more acute ailments contributing to a higher risk of PMI and poorer outcomes compared to cancer patients requiring tracheotomy. We propose routine screening for PMI with cTnI in the postoperative period in all tracheotomy patients.</p>","PeriodicalId":32097,"journal":{"name":"World Journal of OtorhinolaryngologyHead and Neck Surgery","volume":"11 3","pages":"412-416"},"PeriodicalIF":1.4000,"publicationDate":"2024-10-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12418321/pdf/","citationCount":"0","resultStr":"{\"title\":\"Predictors of and outcomes related to perioperative myocardial injury post-tracheotomy.\",\"authors\":\"Randy W Lesh, Jino Park, Vincent M Desiato, Martin Matsumura, Thorsen W Haugen\",\"doi\":\"10.1002/wjo2.218\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Perioperative myocardial injury (PMI) is associated with increased mortality. We describe risk factors for and outcomes of PMI in patients undergoing tracheotomy.</p><p><strong>Methods: </strong>Retrospective study of patients undergoing tracheotomy from 2007 to 2016. PMI was defined by a postoperative cardiac troponin I (cTnI) > 99th percentile. Demographics and comorbidities were extracted from the electronic medical record and compared between patients with and without PMI. Significant univariate predictors were included in a multivariable logistic regression model to determine independent predictors of PMI. Thirty-day and 1-year mortality of patients with and without PMI were compared.</p><p><strong>Results: </strong>Of 861 patients undergoing tracheotomy, 41 (4.76%) had PMI and 820 (95.24%) did not. PMI was associated with higher mortality at both 30 days (40.5% vs. 11.2%, <i>p</i> < 0.001) and 1 year (73.2% vs. 44.1%, <i>p</i> < 0.001). Patients with PMI were older (median age 65 vs. 60, <i>p</i> = 0.002) and more likely to have prior myocardial infarction (MI) (36.6% vs. 10.7%, <i>p</i> < 0.001) and chronic kidney disease (31.7% vs. 16.7%, <i>p</i> = 0.024). Cancer diagnosis was associated with a lower risk of PMI (24.4% vs. 41.8%, <i>p</i> = 0.041). Older age (odds ratio [OR] = 1.033, <i>p</i> < 0.001) and prior MI (OR = 3.686, <i>p</i> < 0.001) were independently associated with PMI.</p><p><strong>Conclusion: </strong>Patients with PMI following tracheotomy had increased short- and long-term mortality. Increased age and history of prior MI were independent predictors of PMI, while cancer was associated with a lower risk of PMI following tracheotomy. ICU patients likely have more acute ailments contributing to a higher risk of PMI and poorer outcomes compared to cancer patients requiring tracheotomy. We propose routine screening for PMI with cTnI in the postoperative period in all tracheotomy patients.</p>\",\"PeriodicalId\":32097,\"journal\":{\"name\":\"World Journal of OtorhinolaryngologyHead and Neck Surgery\",\"volume\":\"11 3\",\"pages\":\"412-416\"},\"PeriodicalIF\":1.4000,\"publicationDate\":\"2024-10-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12418321/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of OtorhinolaryngologyHead and Neck Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/wjo2.218\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of OtorhinolaryngologyHead and Neck Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/wjo2.218","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
围手术期心肌损伤(PMI)与死亡率增加相关。我们描述了气管切开术患者PMI的危险因素和结果。方法:回顾性分析2007 ~ 2016年气管切开术患者的临床资料。PMI的定义是术后心肌肌钙蛋白I (cTnI)的第99个百分位数。从电子病历中提取人口统计数据和合并症,并比较有和没有PMI的患者。在多变量logistic回归模型中纳入显著的单变量预测因子,以确定PMI的独立预测因子。比较有PMI和无PMI患者的30天和1年死亡率。结果:861例气管切开术患者中,41例(4.76%)有PMI, 820例(95.24%)无PMI。PMI与30天内较高的死亡率(40.5%对11.2%,p p = 0.002)和更有可能发生心肌梗死(MI)(36.6%对10.7%,p p = 0.024)相关。癌症诊断与较低的PMI风险相关(24.4%比41.8%,p = 0.041)。结论:气管切开术后PMI患者的短期和长期死亡率均增加。年龄增加和既往心肌梗死史是PMI的独立预测因素,而癌症与气管切开术后PMI的风险降低相关。与需要气管切开术的癌症患者相比,ICU患者可能有更多的急性疾病,导致PMI风险更高,预后更差。我们建议在所有气管切开术患者的术后阶段对PMI和cTnI进行常规筛查。
Predictors of and outcomes related to perioperative myocardial injury post-tracheotomy.
Introduction: Perioperative myocardial injury (PMI) is associated with increased mortality. We describe risk factors for and outcomes of PMI in patients undergoing tracheotomy.
Methods: Retrospective study of patients undergoing tracheotomy from 2007 to 2016. PMI was defined by a postoperative cardiac troponin I (cTnI) > 99th percentile. Demographics and comorbidities were extracted from the electronic medical record and compared between patients with and without PMI. Significant univariate predictors were included in a multivariable logistic regression model to determine independent predictors of PMI. Thirty-day and 1-year mortality of patients with and without PMI were compared.
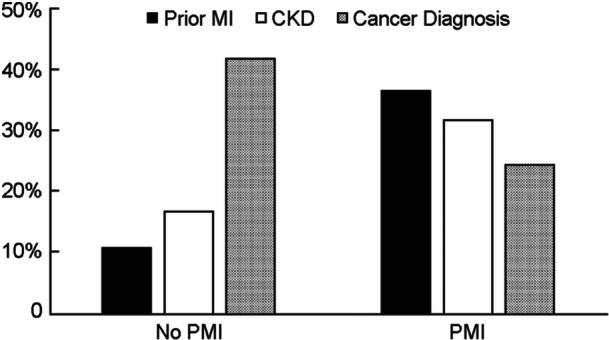
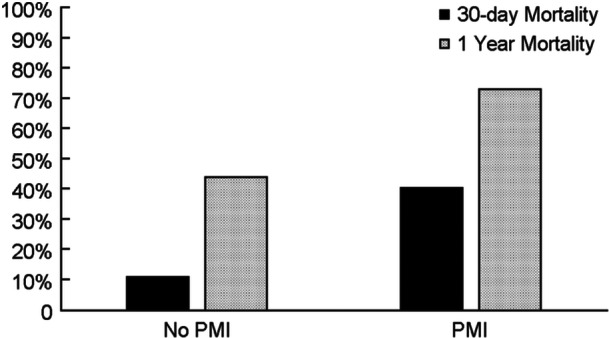
Results: Of 861 patients undergoing tracheotomy, 41 (4.76%) had PMI and 820 (95.24%) did not. PMI was associated with higher mortality at both 30 days (40.5% vs. 11.2%, p < 0.001) and 1 year (73.2% vs. 44.1%, p < 0.001). Patients with PMI were older (median age 65 vs. 60, p = 0.002) and more likely to have prior myocardial infarction (MI) (36.6% vs. 10.7%, p < 0.001) and chronic kidney disease (31.7% vs. 16.7%, p = 0.024). Cancer diagnosis was associated with a lower risk of PMI (24.4% vs. 41.8%, p = 0.041). Older age (odds ratio [OR] = 1.033, p < 0.001) and prior MI (OR = 3.686, p < 0.001) were independently associated with PMI.
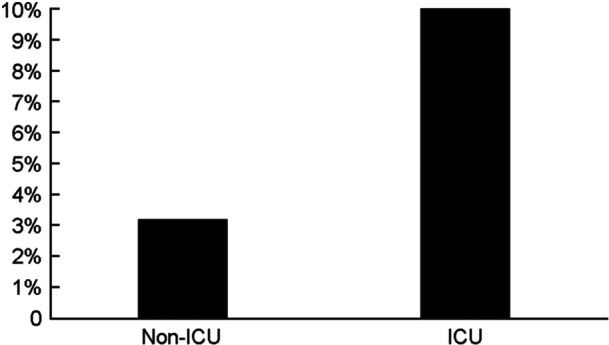
Conclusion: Patients with PMI following tracheotomy had increased short- and long-term mortality. Increased age and history of prior MI were independent predictors of PMI, while cancer was associated with a lower risk of PMI following tracheotomy. ICU patients likely have more acute ailments contributing to a higher risk of PMI and poorer outcomes compared to cancer patients requiring tracheotomy. We propose routine screening for PMI with cTnI in the postoperative period in all tracheotomy patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


