{"title":"肝移植治疗胰十二指肠切除术后代谢功能障碍相关脂肪变性肝病。","authors":"Takeshi Kano, Ryugen Takahashi, Nobuhisa Akamatsu, Yujiro Nishioka, Yuichiro Mihara, Akihiko Ichida, Takeshi Takamoto, Yoshikuni Kawaguchi, Kiyoshi Hasegawa","doi":"10.70352/scrj.cr.25-0264","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Steatotic liver disease (SLD) may develop in some patients after pancreaticoduodenectomy (PD), but no cases requiring liver transplantation (LT) have been reported to date. Here, we present two cases in which LT was performed for decompensated liver cirrhosis (LC) after PD.</p><p><strong>Case presentation: </strong>Case 1 was a 53-year-old man with obesity, metabolic-associated SLD (MASLD), and diabetes mellitus. The patient underwent PD for an intraductal papillary mucinous neoplasm. His liver function worsened and he developed decompensated LC 6 years later, eventually requiring LT. Due to poor mobility of the jejunal limb caused by severe adhesions and the presence of a pancreatojejunostomy, a choledochojejunostomy was performed at the more distal site of the common bile duct than usual. He developed hemobilia and biliary leakage but was discharged on POD 107. Liver function has been good for 2 years after LT without MASLD recurrence, although endoscopic treatment is periodically required for biliary stricture. Case 2 was a 46-year-old man with obesity, SLD, and a history of excessive alcohol consumption. The patient underwent PD for duodenal cancer. Five years later, he developed decompensated LC, which required living-donor LT. For biliary reconstruction, a new jejunal limb was created and elevated. He was discharged on POD 79. He has repeatedly developed cholangitis, but his liver function has been good for 6 years without SLD recurrence.</p><p><strong>Conclusions: </strong>Steatohepatitis can worsen following PD and may lead to decompensated LC, ultimately requiring LT. Therefore, screening for steatohepatitis and its risk factors prior to PD is essential, and prophylaxis should be considered. LT after PD presents surgical challenges and biliary reconstruction with some procedural modifications.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422816/pdf/","citationCount":"0","resultStr":"{\"title\":\"Liver Transplantation for Metabolic Dysfunction-Associated Steatotic Liver Disease after Pancreaticoduodenectomy.\",\"authors\":\"Takeshi Kano, Ryugen Takahashi, Nobuhisa Akamatsu, Yujiro Nishioka, Yuichiro Mihara, Akihiko Ichida, Takeshi Takamoto, Yoshikuni Kawaguchi, Kiyoshi Hasegawa\",\"doi\":\"10.70352/scrj.cr.25-0264\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Steatotic liver disease (SLD) may develop in some patients after pancreaticoduodenectomy (PD), but no cases requiring liver transplantation (LT) have been reported to date. Here, we present two cases in which LT was performed for decompensated liver cirrhosis (LC) after PD.</p><p><strong>Case presentation: </strong>Case 1 was a 53-year-old man with obesity, metabolic-associated SLD (MASLD), and diabetes mellitus. The patient underwent PD for an intraductal papillary mucinous neoplasm. His liver function worsened and he developed decompensated LC 6 years later, eventually requiring LT. Due to poor mobility of the jejunal limb caused by severe adhesions and the presence of a pancreatojejunostomy, a choledochojejunostomy was performed at the more distal site of the common bile duct than usual. He developed hemobilia and biliary leakage but was discharged on POD 107. Liver function has been good for 2 years after LT without MASLD recurrence, although endoscopic treatment is periodically required for biliary stricture. Case 2 was a 46-year-old man with obesity, SLD, and a history of excessive alcohol consumption. The patient underwent PD for duodenal cancer. Five years later, he developed decompensated LC, which required living-donor LT. For biliary reconstruction, a new jejunal limb was created and elevated. He was discharged on POD 79. He has repeatedly developed cholangitis, but his liver function has been good for 6 years without SLD recurrence.</p><p><strong>Conclusions: </strong>Steatohepatitis can worsen following PD and may lead to decompensated LC, ultimately requiring LT. Therefore, screening for steatohepatitis and its risk factors prior to PD is essential, and prophylaxis should be considered. LT after PD presents surgical challenges and biliary reconstruction with some procedural modifications.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12422816/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.25-0264\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0264","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/6 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Liver Transplantation for Metabolic Dysfunction-Associated Steatotic Liver Disease after Pancreaticoduodenectomy.
Introduction: Steatotic liver disease (SLD) may develop in some patients after pancreaticoduodenectomy (PD), but no cases requiring liver transplantation (LT) have been reported to date. Here, we present two cases in which LT was performed for decompensated liver cirrhosis (LC) after PD.
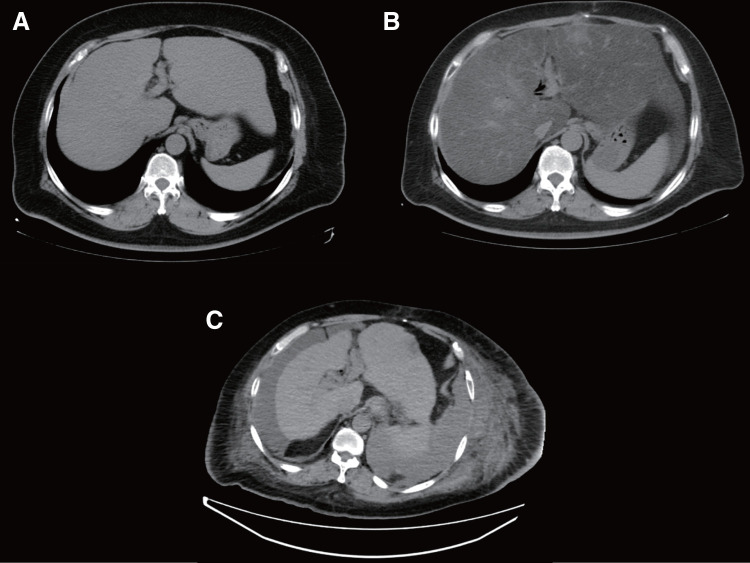
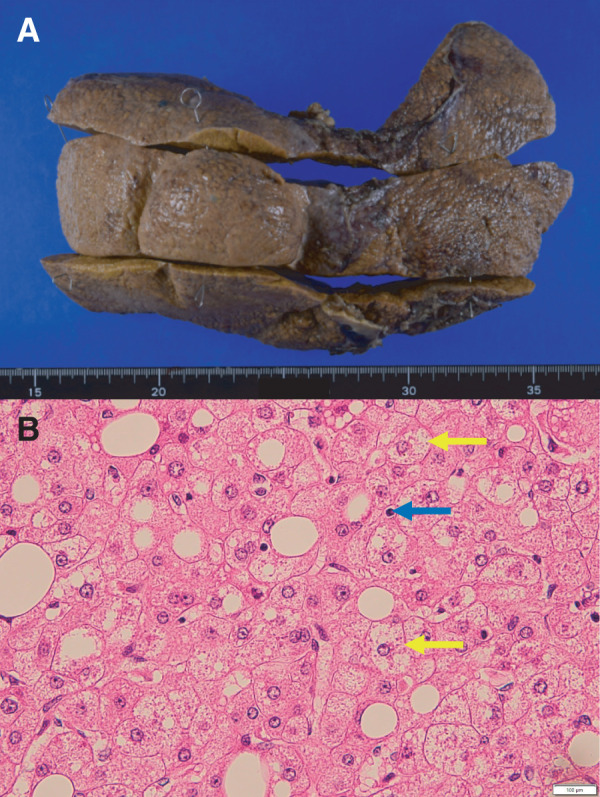
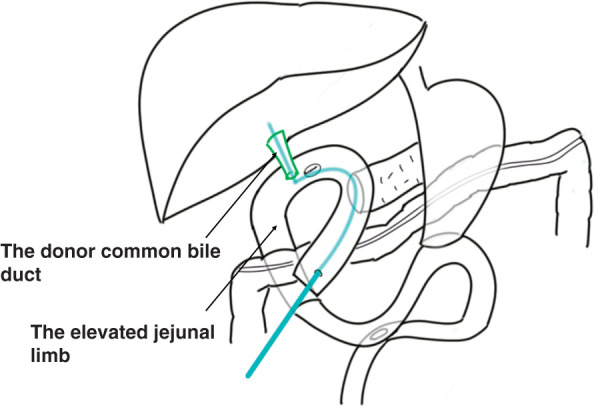
Case presentation: Case 1 was a 53-year-old man with obesity, metabolic-associated SLD (MASLD), and diabetes mellitus. The patient underwent PD for an intraductal papillary mucinous neoplasm. His liver function worsened and he developed decompensated LC 6 years later, eventually requiring LT. Due to poor mobility of the jejunal limb caused by severe adhesions and the presence of a pancreatojejunostomy, a choledochojejunostomy was performed at the more distal site of the common bile duct than usual. He developed hemobilia and biliary leakage but was discharged on POD 107. Liver function has been good for 2 years after LT without MASLD recurrence, although endoscopic treatment is periodically required for biliary stricture. Case 2 was a 46-year-old man with obesity, SLD, and a history of excessive alcohol consumption. The patient underwent PD for duodenal cancer. Five years later, he developed decompensated LC, which required living-donor LT. For biliary reconstruction, a new jejunal limb was created and elevated. He was discharged on POD 79. He has repeatedly developed cholangitis, but his liver function has been good for 6 years without SLD recurrence.
Conclusions: Steatohepatitis can worsen following PD and may lead to decompensated LC, ultimately requiring LT. Therefore, screening for steatohepatitis and its risk factors prior to PD is essential, and prophylaxis should be considered. LT after PD presents surgical challenges and biliary reconstruction with some procedural modifications.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


