Tianzhen Ji, Lei Xie, Tingyu Zhao, Zhengjie Chen, Xiaofen Sun, Yan Zhang, Cheng Xu
{"title":"提高分娩镇痛:低剂量鞘内罗哌卡因-舒芬太尼对脊髓-硬膜外联合镇痛的影响:一项前瞻性双盲随机试验。","authors":"Tianzhen Ji, Lei Xie, Tingyu Zhao, Zhengjie Chen, Xiaofen Sun, Yan Zhang, Cheng Xu","doi":"10.2147/DDDT.S532237","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Combined spinal-epidural (CSE) analgesia delivers rapid labor pain relief, yet high intrathecal opioid doses carry adverse effects, and ultra-low doses shorten block duration. Whether a low intrathecal dose of ropivacaine-sufentanil within CSE reduces clinician-delivered rescue boluses, compared with epidural analgesia (EA) or dural-puncture epidural (DPE), remains unclear.</p><p><strong>Methods: </strong>Laboring women requesting neuraxial analgesia were randomized to three groups: EA, DPE, and CSE. In the CSE group, analgesia was initiated with 2 mL of solution (1 mL 0.1% ropivacaine plus 1 mL containing 1 μg sufentanil), while the EA and DPE groups received 15 mL of 0.09% ropivacaine with 0.4 μg/mL sufentanil. The primary outcome was the proportion of patients requiring supplemental provider-administered analgesia for breakthrough pain. Secondary outcomes included analgesia onset time, VAS scores at multiple time points, patient-controlled epidural analgesia button presses, and cumulative analgesic consumption.</p><p><strong>Results: </strong>A total of 131 women completed the study: 42 (EA), 44 (DPE), and 45 (CSE). After adjusting for age, gestational age, cervical dilation, ASA status, BMI, and baseline VAS, the CSE group showed a significantly lower need for supplemental analgesia compared to EA (22% vs 48%; adjusted odds ratio [aOR]: 0.29, 95% CI: 0.10-0.78; P=0.013). The DPE group (30%) also exhibited a lower incidence than EA, but the difference did not reach significance (aOR: 0.43, 95% CI: 0.16-1.09; P=0.09). Between CSE and DPE, no significant difference emerged (aOR: 0.66, 95% CI: 0.24-1.74; P=0.27). The primary hypothesis that CSE would outperform both EA and DPE was not fully supported. For secondary outcomes, the CSE group demonstrated faster onset and significantly lower VAS scores at prespecified intervals than DPE and EA (P<0.001).</p><p><strong>Conclusion: </strong>Low-dose intrathecal ropivacaine-sufentanil CSE reduced supplemental analgesia needs versus EA but not DPE. Although CSE produced a faster onset and greater sensory block, its superiority over DPE was not established. Thus, CSE and DPE are clinically acceptable, with CSE potentially favored where minimal breakthrough pain is prioritized; further multicenter studies are warranted to confirm these findings.</p><p><strong>Trial registration number: </strong>ChiCTR2300076206. The trial is publicly available and is registered at www.chictr.org.cn on Sept 7, 2023.</p>","PeriodicalId":11290,"journal":{"name":"Drug Design, Development and Therapy","volume":"19 ","pages":"7763-7775"},"PeriodicalIF":5.1000,"publicationDate":"2025-09-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421255/pdf/","citationCount":"0","resultStr":"{\"title\":\"Elevating Labor Analgesia: The Impact of Low-Dose Intrathecal Ropivacaine-Sufentanil in Combined Spinal-Epidural Analgesia: A Prospective Double-Blinded Randomized Trial.\",\"authors\":\"Tianzhen Ji, Lei Xie, Tingyu Zhao, Zhengjie Chen, Xiaofen Sun, Yan Zhang, Cheng Xu\",\"doi\":\"10.2147/DDDT.S532237\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Combined spinal-epidural (CSE) analgesia delivers rapid labor pain relief, yet high intrathecal opioid doses carry adverse effects, and ultra-low doses shorten block duration. Whether a low intrathecal dose of ropivacaine-sufentanil within CSE reduces clinician-delivered rescue boluses, compared with epidural analgesia (EA) or dural-puncture epidural (DPE), remains unclear.</p><p><strong>Methods: </strong>Laboring women requesting neuraxial analgesia were randomized to three groups: EA, DPE, and CSE. In the CSE group, analgesia was initiated with 2 mL of solution (1 mL 0.1% ropivacaine plus 1 mL containing 1 μg sufentanil), while the EA and DPE groups received 15 mL of 0.09% ropivacaine with 0.4 μg/mL sufentanil. The primary outcome was the proportion of patients requiring supplemental provider-administered analgesia for breakthrough pain. Secondary outcomes included analgesia onset time, VAS scores at multiple time points, patient-controlled epidural analgesia button presses, and cumulative analgesic consumption.</p><p><strong>Results: </strong>A total of 131 women completed the study: 42 (EA), 44 (DPE), and 45 (CSE). After adjusting for age, gestational age, cervical dilation, ASA status, BMI, and baseline VAS, the CSE group showed a significantly lower need for supplemental analgesia compared to EA (22% vs 48%; adjusted odds ratio [aOR]: 0.29, 95% CI: 0.10-0.78; P=0.013). The DPE group (30%) also exhibited a lower incidence than EA, but the difference did not reach significance (aOR: 0.43, 95% CI: 0.16-1.09; P=0.09). Between CSE and DPE, no significant difference emerged (aOR: 0.66, 95% CI: 0.24-1.74; P=0.27). The primary hypothesis that CSE would outperform both EA and DPE was not fully supported. For secondary outcomes, the CSE group demonstrated faster onset and significantly lower VAS scores at prespecified intervals than DPE and EA (P<0.001).</p><p><strong>Conclusion: </strong>Low-dose intrathecal ropivacaine-sufentanil CSE reduced supplemental analgesia needs versus EA but not DPE. Although CSE produced a faster onset and greater sensory block, its superiority over DPE was not established. Thus, CSE and DPE are clinically acceptable, with CSE potentially favored where minimal breakthrough pain is prioritized; further multicenter studies are warranted to confirm these findings.</p><p><strong>Trial registration number: </strong>ChiCTR2300076206. The trial is publicly available and is registered at www.chictr.org.cn on Sept 7, 2023.</p>\",\"PeriodicalId\":11290,\"journal\":{\"name\":\"Drug Design, Development and Therapy\",\"volume\":\"19 \",\"pages\":\"7763-7775\"},\"PeriodicalIF\":5.1000,\"publicationDate\":\"2025-09-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421255/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Drug Design, Development and Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/DDDT.S532237\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"CHEMISTRY, MEDICINAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drug Design, Development and Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/DDDT.S532237","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"CHEMISTRY, MEDICINAL","Score":null,"Total":0}
引用次数: 0
摘要
背景:脊髓-硬膜外联合镇痛(CSE)可快速缓解分娩疼痛,但鞘内高剂量阿片类药物会产生不良反应,超低剂量阿片类药物会缩短阻滞持续时间。与硬膜外镇痛(EA)或硬膜外穿刺(DPE)相比,CSE中低剂量的罗哌卡因-舒芬太尼鞘内注射是否会减少临床交付的抢救丸,目前尚不清楚。方法:要求轴向镇痛的分娩妇女随机分为EA组、DPE组和CSE组。CSE组给予2 mL溶液(1 mL 0.1%罗哌卡因加1 mL含1 μg舒芬太尼),EA组和DPE组给予15 mL 0.09%罗哌卡因加0.4 μg/mL舒芬太尼。主要结果是突破性疼痛需要补充的由提供者给药的患者比例。次要结局包括镇痛起效时间、多个时间点的VAS评分、患者控制的硬膜外镇痛按钮按下次数和累计镇痛用量。结果:共有131名女性完成了研究:42名(EA), 44名(DPE)和45名(CSE)。在调整了年龄、胎龄、宫颈扩张、ASA状态、BMI和基线VAS后,与EA组相比,CSE组对补充镇痛的需求明显降低(22% vs 48%;调整优势比[aOR]: 0.29, 95% CI: 0.10-0.78; P=0.013)。DPE组(30%)的发病率也低于EA组,但差异无统计学意义(aOR: 0.43, 95% CI: 0.16-1.09; P=0.09)。CSE与DPE之间无显著差异(aOR: 0.66, 95% CI: 0.24 ~ 1.74; P=0.27)。CSE将优于EA和DPE的主要假设没有得到充分支持。对于次要结局,CSE组比DPE组和EA组表现出更快的起效,并且在预定间隔内VAS评分明显低于DPE组(结论:与EA相比,低剂量鞘内罗哌卡因-舒芬太尼CSE组减少了补充镇痛需求,但DPE组没有。虽然CSE发作更快,感觉阻滞更大,但其优于DPE的优势尚未确定。因此,CSE和DPE在临床上是可接受的,CSE可能优先考虑最小的突破性疼痛;需要进一步的多中心研究来证实这些发现。试验注册号:ChiCTR2300076206。该试验是公开的,并于2023年9月7日在www.chictr.org.cn上注册。
Elevating Labor Analgesia: The Impact of Low-Dose Intrathecal Ropivacaine-Sufentanil in Combined Spinal-Epidural Analgesia: A Prospective Double-Blinded Randomized Trial.
Background: Combined spinal-epidural (CSE) analgesia delivers rapid labor pain relief, yet high intrathecal opioid doses carry adverse effects, and ultra-low doses shorten block duration. Whether a low intrathecal dose of ropivacaine-sufentanil within CSE reduces clinician-delivered rescue boluses, compared with epidural analgesia (EA) or dural-puncture epidural (DPE), remains unclear.
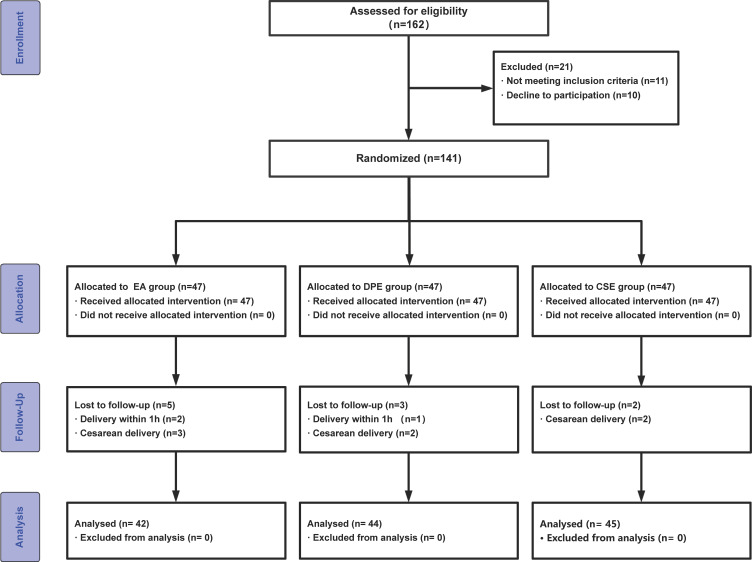
Methods: Laboring women requesting neuraxial analgesia were randomized to three groups: EA, DPE, and CSE. In the CSE group, analgesia was initiated with 2 mL of solution (1 mL 0.1% ropivacaine plus 1 mL containing 1 μg sufentanil), while the EA and DPE groups received 15 mL of 0.09% ropivacaine with 0.4 μg/mL sufentanil. The primary outcome was the proportion of patients requiring supplemental provider-administered analgesia for breakthrough pain. Secondary outcomes included analgesia onset time, VAS scores at multiple time points, patient-controlled epidural analgesia button presses, and cumulative analgesic consumption.
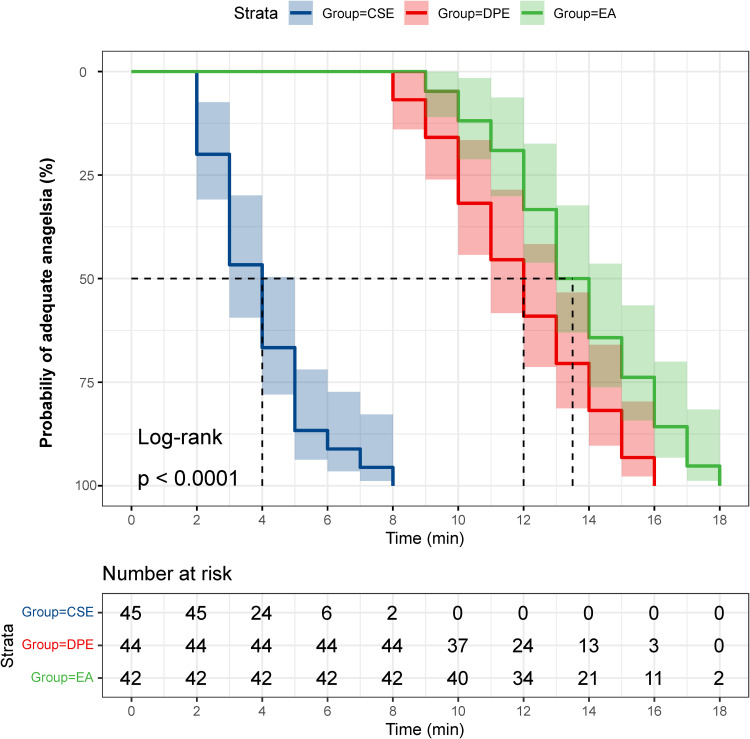
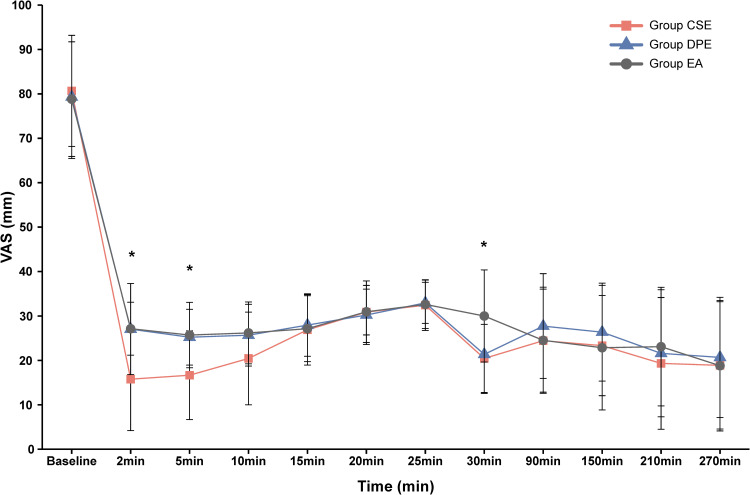
Results: A total of 131 women completed the study: 42 (EA), 44 (DPE), and 45 (CSE). After adjusting for age, gestational age, cervical dilation, ASA status, BMI, and baseline VAS, the CSE group showed a significantly lower need for supplemental analgesia compared to EA (22% vs 48%; adjusted odds ratio [aOR]: 0.29, 95% CI: 0.10-0.78; P=0.013). The DPE group (30%) also exhibited a lower incidence than EA, but the difference did not reach significance (aOR: 0.43, 95% CI: 0.16-1.09; P=0.09). Between CSE and DPE, no significant difference emerged (aOR: 0.66, 95% CI: 0.24-1.74; P=0.27). The primary hypothesis that CSE would outperform both EA and DPE was not fully supported. For secondary outcomes, the CSE group demonstrated faster onset and significantly lower VAS scores at prespecified intervals than DPE and EA (P<0.001).
Conclusion: Low-dose intrathecal ropivacaine-sufentanil CSE reduced supplemental analgesia needs versus EA but not DPE. Although CSE produced a faster onset and greater sensory block, its superiority over DPE was not established. Thus, CSE and DPE are clinically acceptable, with CSE potentially favored where minimal breakthrough pain is prioritized; further multicenter studies are warranted to confirm these findings.
Trial registration number: ChiCTR2300076206. The trial is publicly available and is registered at www.chictr.org.cn on Sept 7, 2023.
期刊介绍:
Drug Design, Development and Therapy is an international, peer-reviewed, open access journal that spans the spectrum of drug design, discovery and development through to clinical applications.
The journal is characterized by the rapid reporting of high-quality original research, reviews, expert opinions, commentary and clinical studies in all therapeutic areas.
Specific topics covered by the journal include:
Drug target identification and validation
Phenotypic screening and target deconvolution
Biochemical analyses of drug targets and their pathways
New methods or relevant applications in molecular/drug design and computer-aided drug discovery*
Design, synthesis, and biological evaluation of novel biologically active compounds (including diagnostics or chemical probes)
Structural or molecular biological studies elucidating molecular recognition processes
Fragment-based drug discovery
Pharmaceutical/red biotechnology
Isolation, structural characterization, (bio)synthesis, bioengineering and pharmacological evaluation of natural products**
Distribution, pharmacokinetics and metabolic transformations of drugs or biologically active compounds in drug development
Drug delivery and formulation (design and characterization of dosage forms, release mechanisms and in vivo testing)
Preclinical development studies
Translational animal models
Mechanisms of action and signalling pathways
Toxicology
Gene therapy, cell therapy and immunotherapy
Personalized medicine and pharmacogenomics
Clinical drug evaluation
Patient safety and sustained use of medicines.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


