Ahmed Nassar, Noha E Aly, Mootaz Elhusseini, Craig Parnaby, Emad Aly
{"title":"同时性直肠癌和前列腺癌的治疗结果:一项系统综述。","authors":"Ahmed Nassar, Noha E Aly, Mootaz Elhusseini, Craig Parnaby, Emad Aly","doi":"10.1007/s00384-025-04992-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The optimal management of synchronous rectal cancer (RC) and prostate cancer (PC) remains unclear. This systematic review evaluates treatment strategies and reports postoperative, oncological, and quality-of-life outcomes in patients treated with curative intent.</p><p><strong>Methods: </strong>Following PRISMA guidelines, this systematic review was registered in PROSPERO (CRD42024598049). A search of Ovid MEDLINE, Embase, CENTRAL, and CDSR (inception to February 2025) identified randomised controlled trials and observational studies on synchronous RC and PC. Synchronous disease was defined as diagnosis or treatment initiation within 12 months. Patients with incurable RC were excluded. Treatment strategies and surgical approaches were analysed, with postoperative, oncological, and survival outcomes assessed.</p><p><strong>Results: </strong>Eight retrospective studies (124 patients) were included. Common treatments included pelvic chemoradiotherapy (CRT) followed by surgery (29%), prostate booster radiotherapy with CRT (24.2%), prostate brachytherapy (8%), and no prostate-directed treatment (11.3%). Surgical approaches included total mesorectal excision (TME) (74.4%), TME with prostatectomy (10.8%), and en-bloc pelvic exenteration (8%). Primary anastomosis was achieved in 61.8%, with 70% requiring a diverting stoma. Anastomotic leaks occurred in 10.8%, and severe complications (grades 3b-5) affected 15.4%, with fewer in robotic-assisted surgery (8.3%). R0 resection was achieved in 92.8%, with no difference between robotic and non-robotic groups. Local recurrence and distant metastasis occurred in 5.9% and 27%, respectively.</p><p><strong>Conclusion: </strong>There is no consistent approach for managing synchronous RC and PC. High-dose prostate radiotherapy may not improve survival and may increase postoperative complications. Robotic-assisted resections may reduce major complications without compromising oncological outcomes.</p>","PeriodicalId":13789,"journal":{"name":"International Journal of Colorectal Disease","volume":"40 1","pages":"195"},"PeriodicalIF":2.3000,"publicationDate":"2025-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12423125/pdf/","citationCount":"0","resultStr":"{\"title\":\"Outcomes of the management of synchronous rectal and prostate cancer: a systematic review.\",\"authors\":\"Ahmed Nassar, Noha E Aly, Mootaz Elhusseini, Craig Parnaby, Emad Aly\",\"doi\":\"10.1007/s00384-025-04992-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The optimal management of synchronous rectal cancer (RC) and prostate cancer (PC) remains unclear. This systematic review evaluates treatment strategies and reports postoperative, oncological, and quality-of-life outcomes in patients treated with curative intent.</p><p><strong>Methods: </strong>Following PRISMA guidelines, this systematic review was registered in PROSPERO (CRD42024598049). A search of Ovid MEDLINE, Embase, CENTRAL, and CDSR (inception to February 2025) identified randomised controlled trials and observational studies on synchronous RC and PC. Synchronous disease was defined as diagnosis or treatment initiation within 12 months. Patients with incurable RC were excluded. Treatment strategies and surgical approaches were analysed, with postoperative, oncological, and survival outcomes assessed.</p><p><strong>Results: </strong>Eight retrospective studies (124 patients) were included. Common treatments included pelvic chemoradiotherapy (CRT) followed by surgery (29%), prostate booster radiotherapy with CRT (24.2%), prostate brachytherapy (8%), and no prostate-directed treatment (11.3%). Surgical approaches included total mesorectal excision (TME) (74.4%), TME with prostatectomy (10.8%), and en-bloc pelvic exenteration (8%). Primary anastomosis was achieved in 61.8%, with 70% requiring a diverting stoma. Anastomotic leaks occurred in 10.8%, and severe complications (grades 3b-5) affected 15.4%, with fewer in robotic-assisted surgery (8.3%). R0 resection was achieved in 92.8%, with no difference between robotic and non-robotic groups. Local recurrence and distant metastasis occurred in 5.9% and 27%, respectively.</p><p><strong>Conclusion: </strong>There is no consistent approach for managing synchronous RC and PC. High-dose prostate radiotherapy may not improve survival and may increase postoperative complications. Robotic-assisted resections may reduce major complications without compromising oncological outcomes.</p>\",\"PeriodicalId\":13789,\"journal\":{\"name\":\"International Journal of Colorectal Disease\",\"volume\":\"40 1\",\"pages\":\"195\"},\"PeriodicalIF\":2.3000,\"publicationDate\":\"2025-09-11\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12423125/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Colorectal Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s00384-025-04992-w\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00384-025-04992-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Outcomes of the management of synchronous rectal and prostate cancer: a systematic review.
Background: The optimal management of synchronous rectal cancer (RC) and prostate cancer (PC) remains unclear. This systematic review evaluates treatment strategies and reports postoperative, oncological, and quality-of-life outcomes in patients treated with curative intent.
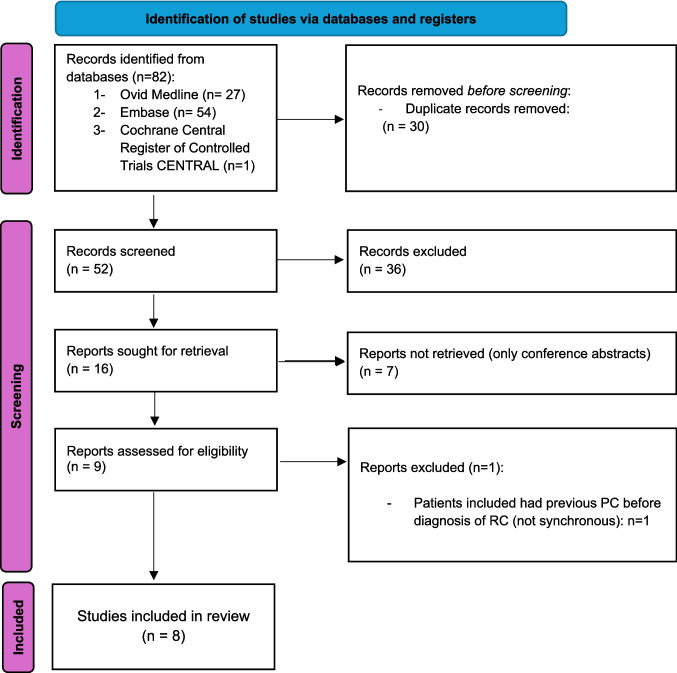
Methods: Following PRISMA guidelines, this systematic review was registered in PROSPERO (CRD42024598049). A search of Ovid MEDLINE, Embase, CENTRAL, and CDSR (inception to February 2025) identified randomised controlled trials and observational studies on synchronous RC and PC. Synchronous disease was defined as diagnosis or treatment initiation within 12 months. Patients with incurable RC were excluded. Treatment strategies and surgical approaches were analysed, with postoperative, oncological, and survival outcomes assessed.
Results: Eight retrospective studies (124 patients) were included. Common treatments included pelvic chemoradiotherapy (CRT) followed by surgery (29%), prostate booster radiotherapy with CRT (24.2%), prostate brachytherapy (8%), and no prostate-directed treatment (11.3%). Surgical approaches included total mesorectal excision (TME) (74.4%), TME with prostatectomy (10.8%), and en-bloc pelvic exenteration (8%). Primary anastomosis was achieved in 61.8%, with 70% requiring a diverting stoma. Anastomotic leaks occurred in 10.8%, and severe complications (grades 3b-5) affected 15.4%, with fewer in robotic-assisted surgery (8.3%). R0 resection was achieved in 92.8%, with no difference between robotic and non-robotic groups. Local recurrence and distant metastasis occurred in 5.9% and 27%, respectively.
Conclusion: There is no consistent approach for managing synchronous RC and PC. High-dose prostate radiotherapy may not improve survival and may increase postoperative complications. Robotic-assisted resections may reduce major complications without compromising oncological outcomes.
期刊介绍:
The International Journal of Colorectal Disease, Clinical and Molecular Gastroenterology and Surgery aims to publish novel and state-of-the-art papers which deal with the physiology and pathophysiology of diseases involving the entire gastrointestinal tract. In addition to original research articles, the following categories will be included: reviews (usually commissioned but may also be submitted), case reports, letters to the editor, and protocols on clinical studies.
The journal offers its readers an interdisciplinary forum for clinical science and molecular research related to gastrointestinal disease.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


