Sarah Elizabeth Alland, Bianca Mills, Michelle Bolte, Colleen Ma, Sally Munnoch, Matthew Kelly
{"title":"澳大利亚一家地区医院艰难梭菌感染和抗生素处方:一项病例对照研究。","authors":"Sarah Elizabeth Alland, Bianca Mills, Michelle Bolte, Colleen Ma, Sally Munnoch, Matthew Kelly","doi":"10.1017/ash.2025.10113","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong><i>Clostridioides difficile</i> infections (CDI) increased at a large, regional hospital in New South Wales, Australia, in 2021, coinciding with an increase at hospitals Australia wide. We aimed to investigate the association between antibiotic prescribing practices and hospital-acquired CDI at the hospital to inform antimicrobial stewardship (AMS) programs.</p><p><strong>Methods: </strong>We conducted a retrospective case-control study for the period July 1, 2018, and June 30, 2022. Seventy hospital-acquired CDI cases were selected for the study. Cases were matched on a 1:2 basis with randomly selected controls based on date of hospitalization and age group. We conducted a multivariable analysis to explore possible risk factors for infection. We compared cases and controls who were administered antibiotics to determine if rates of inappropriate antibiotic prescriptions differed between cases and controls.</p><p><strong>Results: </strong>The multivariable model found that use of cephalosporins (third, fourth, or fifth generation) (adjusted odds ratio (aOR) 3.82, 95% confidence interval (CI) 1.35-10.84), use of penicillins (broad or extended broad spectrum) (aOR 5.79, 95% CI 2.15-15.58), and increased complexity of comorbidities (aOR 1.22, 95% CI 1.02-1.45) were independently associated with CDI. In patients who had antibiotics administered during their admission, inappropriate antibiotic prescribing (OR 5.68, 95% CI 1.95-16.48) and non-compliance with antibiotic prescribing guidelines (OR 5.01, 95% CI 1.07-14.76) were associated with CDI.</p><p><strong>Conclusions: </strong>Our study showed that antibiotic prescribing practices were associated with hospital-acquired CDI at the hospital during the study period. The results reinforce the importance of compliance with antibiotic guidelines and provide further evidence for AMS programs to reduce CDI.</p>","PeriodicalId":72246,"journal":{"name":"Antimicrobial stewardship & healthcare epidemiology : ASHE","volume":"5 1","pages":"e198"},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415799/pdf/","citationCount":"0","resultStr":"{\"title\":\"<i>Clostridioides difficile</i> infection and antibiotic prescribing at a regional hospital in Australia: a case-control study.\",\"authors\":\"Sarah Elizabeth Alland, Bianca Mills, Michelle Bolte, Colleen Ma, Sally Munnoch, Matthew Kelly\",\"doi\":\"10.1017/ash.2025.10113\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong><i>Clostridioides difficile</i> infections (CDI) increased at a large, regional hospital in New South Wales, Australia, in 2021, coinciding with an increase at hospitals Australia wide. We aimed to investigate the association between antibiotic prescribing practices and hospital-acquired CDI at the hospital to inform antimicrobial stewardship (AMS) programs.</p><p><strong>Methods: </strong>We conducted a retrospective case-control study for the period July 1, 2018, and June 30, 2022. Seventy hospital-acquired CDI cases were selected for the study. Cases were matched on a 1:2 basis with randomly selected controls based on date of hospitalization and age group. We conducted a multivariable analysis to explore possible risk factors for infection. We compared cases and controls who were administered antibiotics to determine if rates of inappropriate antibiotic prescriptions differed between cases and controls.</p><p><strong>Results: </strong>The multivariable model found that use of cephalosporins (third, fourth, or fifth generation) (adjusted odds ratio (aOR) 3.82, 95% confidence interval (CI) 1.35-10.84), use of penicillins (broad or extended broad spectrum) (aOR 5.79, 95% CI 2.15-15.58), and increased complexity of comorbidities (aOR 1.22, 95% CI 1.02-1.45) were independently associated with CDI. In patients who had antibiotics administered during their admission, inappropriate antibiotic prescribing (OR 5.68, 95% CI 1.95-16.48) and non-compliance with antibiotic prescribing guidelines (OR 5.01, 95% CI 1.07-14.76) were associated with CDI.</p><p><strong>Conclusions: </strong>Our study showed that antibiotic prescribing practices were associated with hospital-acquired CDI at the hospital during the study period. The results reinforce the importance of compliance with antibiotic guidelines and provide further evidence for AMS programs to reduce CDI.</p>\",\"PeriodicalId\":72246,\"journal\":{\"name\":\"Antimicrobial stewardship & healthcare epidemiology : ASHE\",\"volume\":\"5 1\",\"pages\":\"e198\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415799/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Antimicrobial stewardship & healthcare epidemiology : ASHE\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1017/ash.2025.10113\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Antimicrobial stewardship & healthcare epidemiology : ASHE","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/ash.2025.10113","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:2021年,澳大利亚新南威尔士州一家大型地区医院的艰难梭菌感染(CDI)增加,与澳大利亚各地医院的增加相一致。我们旨在调查医院抗生素处方实践与医院获得性CDI之间的关系,为抗菌药物管理(AMS)计划提供信息。方法:我们在2018年7月1日至2022年6月30日期间进行了回顾性病例对照研究。选取70例医院获得性CDI病例进行研究。病例按1:2的比例与根据住院日期和年龄组随机选择的对照进行匹配。我们进行了多变量分析,以探索可能的感染危险因素。我们比较了使用抗生素的病例和对照组,以确定病例和对照组之间不适当抗生素处方的发生率是否存在差异。结果:多变量模型发现,头孢菌素(第三代、第四代或第五代)的使用(调整优势比(aOR) 3.82, 95%可信区间(CI) 1.35-10.84)、青霉素类药物(广谱或扩展广谱)的使用(aOR 5.79, 95% CI 2.15-15.58)和并发症复杂性的增加(aOR 1.22, 95% CI 1.02-1.45)与CDI独立相关。在入院时使用抗生素的患者中,不适当的抗生素处方(OR 5.68, 95% CI 1.95-16.48)和不遵守抗生素处方指南(OR 5.01, 95% CI 1.07-14.76)与CDI相关。结论:我们的研究表明,在研究期间,医院的抗生素处方实践与医院获得性CDI有关。结果强调了遵守抗生素指南的重要性,并为AMS项目减少CDI提供了进一步的证据。
Clostridioides difficile infection and antibiotic prescribing at a regional hospital in Australia: a case-control study.
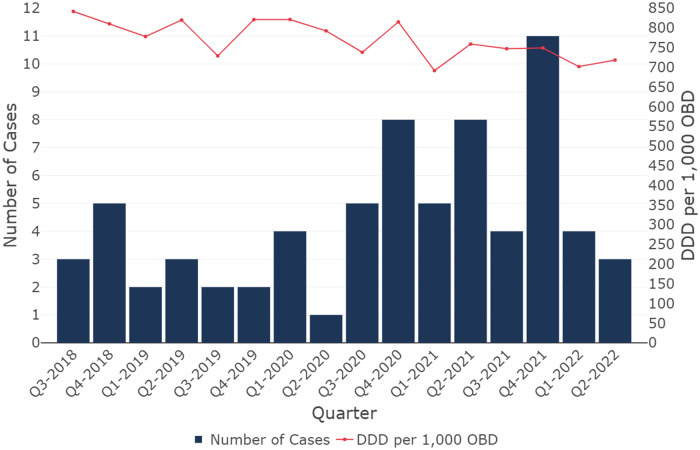
Background: Clostridioides difficile infections (CDI) increased at a large, regional hospital in New South Wales, Australia, in 2021, coinciding with an increase at hospitals Australia wide. We aimed to investigate the association between antibiotic prescribing practices and hospital-acquired CDI at the hospital to inform antimicrobial stewardship (AMS) programs.
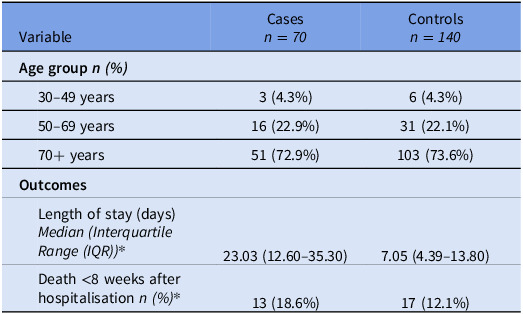
Methods: We conducted a retrospective case-control study for the period July 1, 2018, and June 30, 2022. Seventy hospital-acquired CDI cases were selected for the study. Cases were matched on a 1:2 basis with randomly selected controls based on date of hospitalization and age group. We conducted a multivariable analysis to explore possible risk factors for infection. We compared cases and controls who were administered antibiotics to determine if rates of inappropriate antibiotic prescriptions differed between cases and controls.
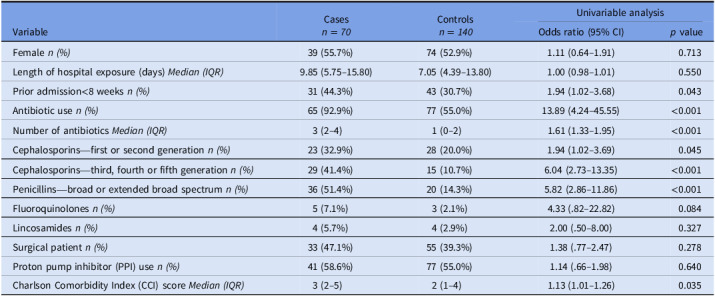
Results: The multivariable model found that use of cephalosporins (third, fourth, or fifth generation) (adjusted odds ratio (aOR) 3.82, 95% confidence interval (CI) 1.35-10.84), use of penicillins (broad or extended broad spectrum) (aOR 5.79, 95% CI 2.15-15.58), and increased complexity of comorbidities (aOR 1.22, 95% CI 1.02-1.45) were independently associated with CDI. In patients who had antibiotics administered during their admission, inappropriate antibiotic prescribing (OR 5.68, 95% CI 1.95-16.48) and non-compliance with antibiotic prescribing guidelines (OR 5.01, 95% CI 1.07-14.76) were associated with CDI.
Conclusions: Our study showed that antibiotic prescribing practices were associated with hospital-acquired CDI at the hospital during the study period. The results reinforce the importance of compliance with antibiotic guidelines and provide further evidence for AMS programs to reduce CDI.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


