Jose Portolés, Rainer Oberbauer, Michele F Eisenga, Aleix Cases, Jolanta Małyszko, Gabriel Choukroun, Marta Crespo, Kai-Uwe Eckardt, Roberto Minutolo
{"title":"肾移植后贫血和缺铁:一个未解决的挑战。","authors":"Jose Portolés, Rainer Oberbauer, Michele F Eisenga, Aleix Cases, Jolanta Małyszko, Gabriel Choukroun, Marta Crespo, Kai-Uwe Eckardt, Roberto Minutolo","doi":"10.1093/ckj/sfaf252","DOIUrl":null,"url":null,"abstract":"<p><p>Anemia and iron deficiency (ID) are common and significant complications in kidney transplant recipients (KTRs) that can affect their health-related quality of life (HRQoL) and outcomes. Current anemia guidelines equate the post-transplant situation with the anemia associated with chronic kidney disease (CKD) in non-transplanted persons, not acknowledging relevant differences ranging from pathophysiology to clinical manifestation. Nephrologists caring for these patients tend to pay less attention to post-transplant anemia (PTA) and ID than in non-transplanted persons with CKD. In this narrative review we summarize the available evidence about PTA and ID and their specifics in KTRs, including associations with patient and graft survival and poorer HRQoL. The prevalence of anemia is higher in KTRs than in non-transplanted patients with CKD for a given level of glomerular filtration rate (GFR) due to kidney transplant (KT)-specific pathophysiological factors. ID should be detected and corrected in KTRs using oral or intravenous (IV) iron. Some IV iron formulations are associated with an increased risk of hypophosphatemia a typical complication in KTRs. Current guidelines suggest the same hemoglobin targets for erythropoiesis stimulating agent therapy in transplanted and non-transplanted patients, despite the fact that a higher hemoglobin target has been associated with a slower estimated GFR decline in KT. There are insufficient data to recommend the widespread use of hypoxia-inducible factor-prolyl-hydroxylase inhibitors in PTA. Red blood cell transfusions should be avoided to minimize alosensitization. We call for increased awareness and targeted trials on anemia and ID in KTRs, accounting for the diverse and specific profiles of these patients.</p>","PeriodicalId":10435,"journal":{"name":"Clinical Kidney Journal","volume":"18 9","pages":"sfaf252"},"PeriodicalIF":4.6000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415517/pdf/","citationCount":"0","resultStr":"{\"title\":\"Anemia and iron deficiency in post-kidney transplantation: an unsolved challenge.\",\"authors\":\"Jose Portolés, Rainer Oberbauer, Michele F Eisenga, Aleix Cases, Jolanta Małyszko, Gabriel Choukroun, Marta Crespo, Kai-Uwe Eckardt, Roberto Minutolo\",\"doi\":\"10.1093/ckj/sfaf252\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Anemia and iron deficiency (ID) are common and significant complications in kidney transplant recipients (KTRs) that can affect their health-related quality of life (HRQoL) and outcomes. Current anemia guidelines equate the post-transplant situation with the anemia associated with chronic kidney disease (CKD) in non-transplanted persons, not acknowledging relevant differences ranging from pathophysiology to clinical manifestation. Nephrologists caring for these patients tend to pay less attention to post-transplant anemia (PTA) and ID than in non-transplanted persons with CKD. In this narrative review we summarize the available evidence about PTA and ID and their specifics in KTRs, including associations with patient and graft survival and poorer HRQoL. The prevalence of anemia is higher in KTRs than in non-transplanted patients with CKD for a given level of glomerular filtration rate (GFR) due to kidney transplant (KT)-specific pathophysiological factors. ID should be detected and corrected in KTRs using oral or intravenous (IV) iron. Some IV iron formulations are associated with an increased risk of hypophosphatemia a typical complication in KTRs. Current guidelines suggest the same hemoglobin targets for erythropoiesis stimulating agent therapy in transplanted and non-transplanted patients, despite the fact that a higher hemoglobin target has been associated with a slower estimated GFR decline in KT. There are insufficient data to recommend the widespread use of hypoxia-inducible factor-prolyl-hydroxylase inhibitors in PTA. Red blood cell transfusions should be avoided to minimize alosensitization. We call for increased awareness and targeted trials on anemia and ID in KTRs, accounting for the diverse and specific profiles of these patients.</p>\",\"PeriodicalId\":10435,\"journal\":{\"name\":\"Clinical Kidney Journal\",\"volume\":\"18 9\",\"pages\":\"sfaf252\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415517/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinical Kidney Journal\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ckj/sfaf252\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Kidney Journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ckj/sfaf252","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Anemia and iron deficiency in post-kidney transplantation: an unsolved challenge.
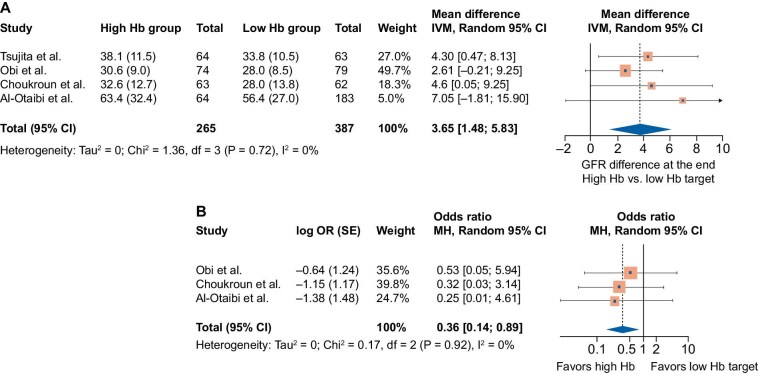
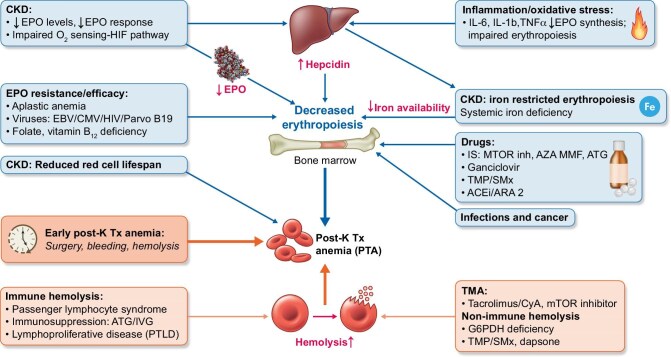
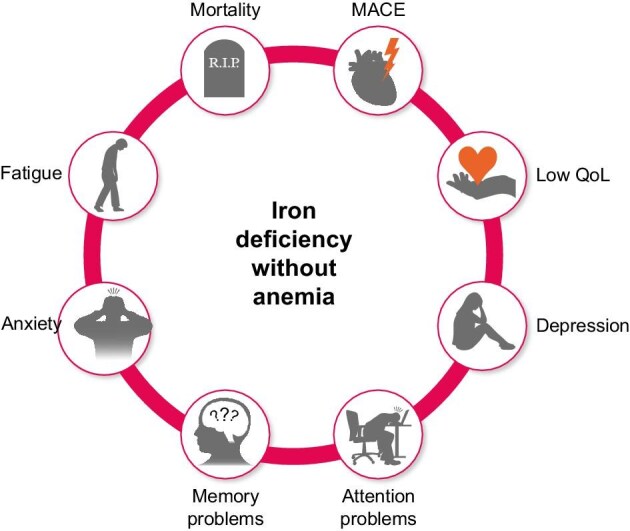
Anemia and iron deficiency (ID) are common and significant complications in kidney transplant recipients (KTRs) that can affect their health-related quality of life (HRQoL) and outcomes. Current anemia guidelines equate the post-transplant situation with the anemia associated with chronic kidney disease (CKD) in non-transplanted persons, not acknowledging relevant differences ranging from pathophysiology to clinical manifestation. Nephrologists caring for these patients tend to pay less attention to post-transplant anemia (PTA) and ID than in non-transplanted persons with CKD. In this narrative review we summarize the available evidence about PTA and ID and their specifics in KTRs, including associations with patient and graft survival and poorer HRQoL. The prevalence of anemia is higher in KTRs than in non-transplanted patients with CKD for a given level of glomerular filtration rate (GFR) due to kidney transplant (KT)-specific pathophysiological factors. ID should be detected and corrected in KTRs using oral or intravenous (IV) iron. Some IV iron formulations are associated with an increased risk of hypophosphatemia a typical complication in KTRs. Current guidelines suggest the same hemoglobin targets for erythropoiesis stimulating agent therapy in transplanted and non-transplanted patients, despite the fact that a higher hemoglobin target has been associated with a slower estimated GFR decline in KT. There are insufficient data to recommend the widespread use of hypoxia-inducible factor-prolyl-hydroxylase inhibitors in PTA. Red blood cell transfusions should be avoided to minimize alosensitization. We call for increased awareness and targeted trials on anemia and ID in KTRs, accounting for the diverse and specific profiles of these patients.
期刊介绍:
About the Journal
Clinical Kidney Journal: Clinical and Translational Nephrology (ckj), an official journal of the ERA-EDTA (European Renal Association-European Dialysis and Transplant Association), is a fully open access, online only journal publishing bimonthly. The journal is an essential educational and training resource integrating clinical, translational and educational research into clinical practice. ckj aims to contribute to a translational research culture among nephrologists and kidney pathologists that helps close the gap between basic researchers and practicing clinicians and promote sorely needed innovation in the Nephrology field. All research articles in this journal have undergone peer review.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


