{"title":"多中心发展预测肺癌脑转移患者生存的临床-分子Nomogram。","authors":"Xiansheng Qiu, Zhenwei Lu, Chongfei Li, Sifang Chen, Xiaoping Zhou, Zhizhu Peng, Li Chen, Wen Peng Zhao, JingJing Shi, Jiawei He, Xuewei Xia, Zhanxiang Wang","doi":"10.2147/CMAR.S538752","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Lung cancer brain metastasis (LCBM) accounts for 40-50% of intracranial malignancies, with emerging evidence of alternative metastatic pathways circumventing the blood-brain barrier. Existing prognostic models lack validation in Asian populations and molecular stratification. This multicenter study aimed to develop a clinical nomogram integrating clinicopathological and molecular determinants for personalized LCBM management.</p><p><strong>Methods: </strong>Retrospective analysis of 522 surgically treated LCBM patients (2015-2021) from four Chinese institutions was conducted. Patients were randomized 7:3 into training (n=365) and validation (n=157) cohorts. Multivariate Cox regression identified independent prognostic factors, which were incorporated into a nomogram predicting 6-/12-/18-month overall survival (OS). Model performance was assessed via time-dependent ROC curves (AUC), calibration plots, and decision curve analysis (DCA).</p><p><strong>Results: </strong>The median OS after neurosurgery was 9 months (range: 4-18 months), with 6-, 12-, and 18-month survival rates of 86.2%, 46.7%, and 17.2%, respectively. Independent predictive factors included brain metastasis size ≥5 cm, Leptomeningeal metastasis(LM), EGFR mutation with TKI treatment, and extracranial metastases. The nomogram demonstrated robust discriminative ability and calibration. EGFR-mutant patients receiving postoperative TKIs showed significantly prolonged survival attributable to enhanced blood-brain barrier permeability. Finally, the authors developed a web-based dynamic nomogram for LCBM patients to facilitate clinical implementation.</p><p><strong>Conclusion: </strong>This study establishes a validated prognostic model integrating tumor burden, EGFR mutation status, and metastatic patterns. It demonstrates that EGFR-guided TKI therapy and bone metastasis surveillance critically influence LCBM outcomes. The nomogram provides a quantifiable framework for risk-adapted therapeutic decisions, advancing precision oncology in neuro-oncology practice.</p>","PeriodicalId":9479,"journal":{"name":"Cancer Management and Research","volume":"17 ","pages":"1881-1895"},"PeriodicalIF":2.6000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415090/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multicenter Development of a Clinical-Molecular Nomogram for Predicting Survival in Lung Cancer Brain Metastasis Patients.\",\"authors\":\"Xiansheng Qiu, Zhenwei Lu, Chongfei Li, Sifang Chen, Xiaoping Zhou, Zhizhu Peng, Li Chen, Wen Peng Zhao, JingJing Shi, Jiawei He, Xuewei Xia, Zhanxiang Wang\",\"doi\":\"10.2147/CMAR.S538752\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Lung cancer brain metastasis (LCBM) accounts for 40-50% of intracranial malignancies, with emerging evidence of alternative metastatic pathways circumventing the blood-brain barrier. Existing prognostic models lack validation in Asian populations and molecular stratification. This multicenter study aimed to develop a clinical nomogram integrating clinicopathological and molecular determinants for personalized LCBM management.</p><p><strong>Methods: </strong>Retrospective analysis of 522 surgically treated LCBM patients (2015-2021) from four Chinese institutions was conducted. Patients were randomized 7:3 into training (n=365) and validation (n=157) cohorts. Multivariate Cox regression identified independent prognostic factors, which were incorporated into a nomogram predicting 6-/12-/18-month overall survival (OS). Model performance was assessed via time-dependent ROC curves (AUC), calibration plots, and decision curve analysis (DCA).</p><p><strong>Results: </strong>The median OS after neurosurgery was 9 months (range: 4-18 months), with 6-, 12-, and 18-month survival rates of 86.2%, 46.7%, and 17.2%, respectively. Independent predictive factors included brain metastasis size ≥5 cm, Leptomeningeal metastasis(LM), EGFR mutation with TKI treatment, and extracranial metastases. The nomogram demonstrated robust discriminative ability and calibration. EGFR-mutant patients receiving postoperative TKIs showed significantly prolonged survival attributable to enhanced blood-brain barrier permeability. Finally, the authors developed a web-based dynamic nomogram for LCBM patients to facilitate clinical implementation.</p><p><strong>Conclusion: </strong>This study establishes a validated prognostic model integrating tumor burden, EGFR mutation status, and metastatic patterns. It demonstrates that EGFR-guided TKI therapy and bone metastasis surveillance critically influence LCBM outcomes. The nomogram provides a quantifiable framework for risk-adapted therapeutic decisions, advancing precision oncology in neuro-oncology practice.</p>\",\"PeriodicalId\":9479,\"journal\":{\"name\":\"Cancer Management and Research\",\"volume\":\"17 \",\"pages\":\"1881-1895\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2025-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12415090/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Management and Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.2147/CMAR.S538752\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Management and Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CMAR.S538752","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
Multicenter Development of a Clinical-Molecular Nomogram for Predicting Survival in Lung Cancer Brain Metastasis Patients.
Background: Lung cancer brain metastasis (LCBM) accounts for 40-50% of intracranial malignancies, with emerging evidence of alternative metastatic pathways circumventing the blood-brain barrier. Existing prognostic models lack validation in Asian populations and molecular stratification. This multicenter study aimed to develop a clinical nomogram integrating clinicopathological and molecular determinants for personalized LCBM management.
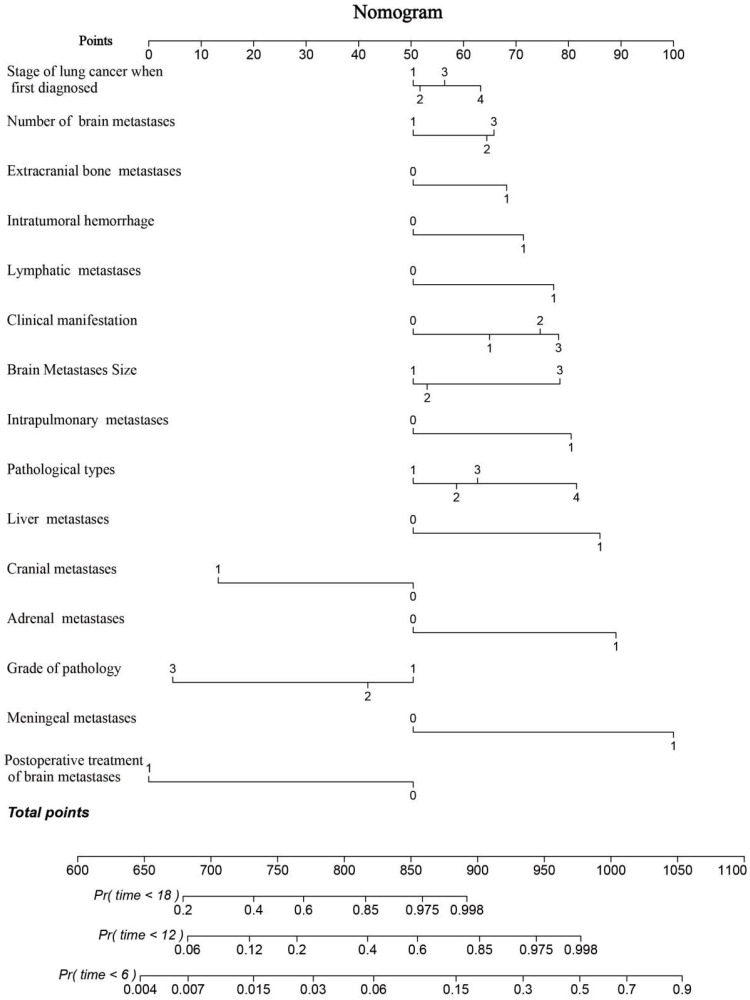
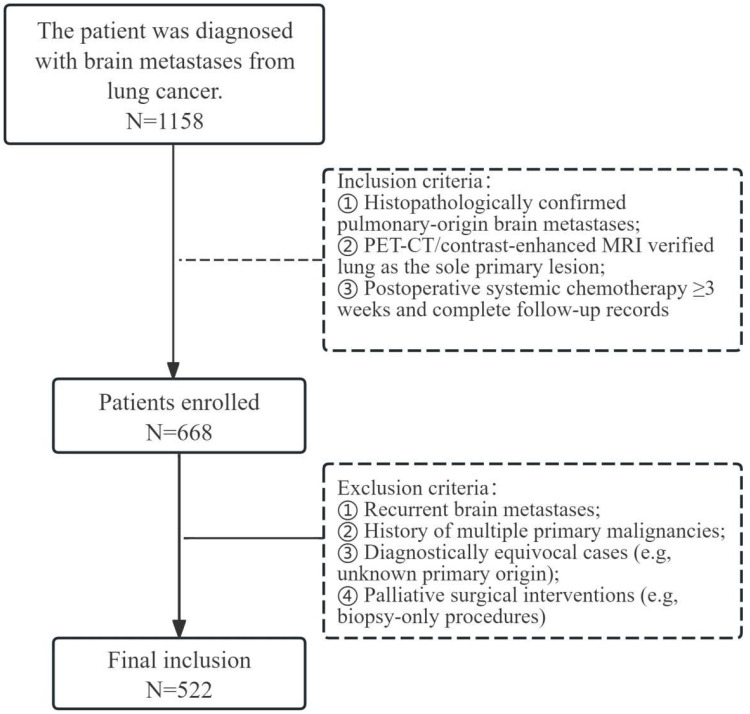
Methods: Retrospective analysis of 522 surgically treated LCBM patients (2015-2021) from four Chinese institutions was conducted. Patients were randomized 7:3 into training (n=365) and validation (n=157) cohorts. Multivariate Cox regression identified independent prognostic factors, which were incorporated into a nomogram predicting 6-/12-/18-month overall survival (OS). Model performance was assessed via time-dependent ROC curves (AUC), calibration plots, and decision curve analysis (DCA).
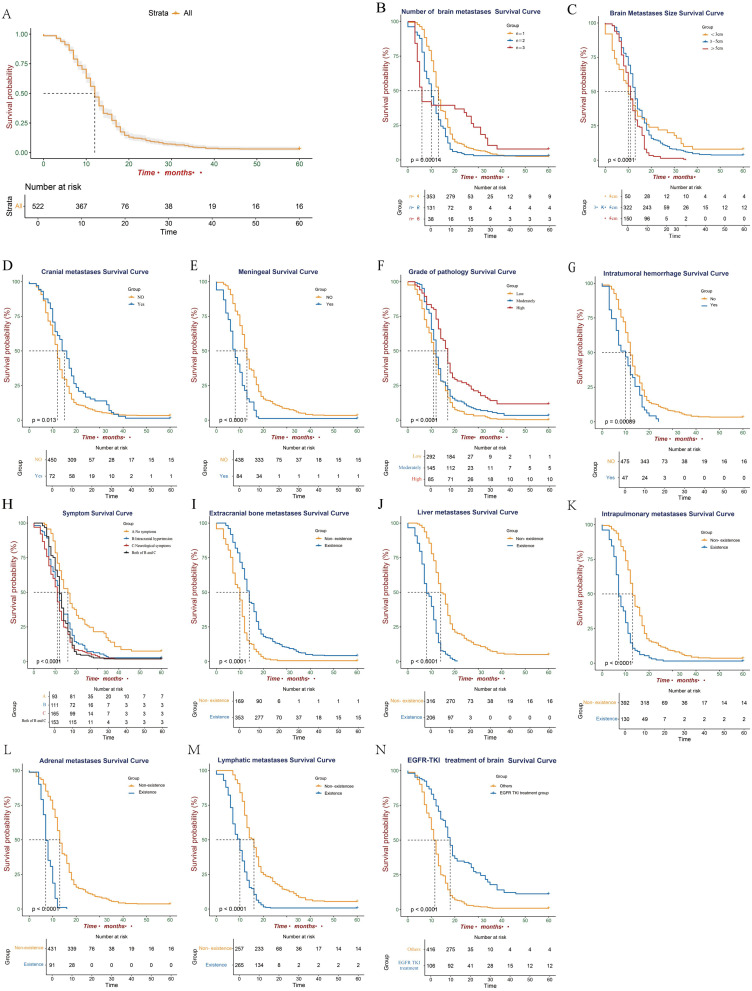
Results: The median OS after neurosurgery was 9 months (range: 4-18 months), with 6-, 12-, and 18-month survival rates of 86.2%, 46.7%, and 17.2%, respectively. Independent predictive factors included brain metastasis size ≥5 cm, Leptomeningeal metastasis(LM), EGFR mutation with TKI treatment, and extracranial metastases. The nomogram demonstrated robust discriminative ability and calibration. EGFR-mutant patients receiving postoperative TKIs showed significantly prolonged survival attributable to enhanced blood-brain barrier permeability. Finally, the authors developed a web-based dynamic nomogram for LCBM patients to facilitate clinical implementation.
Conclusion: This study establishes a validated prognostic model integrating tumor burden, EGFR mutation status, and metastatic patterns. It demonstrates that EGFR-guided TKI therapy and bone metastasis surveillance critically influence LCBM outcomes. The nomogram provides a quantifiable framework for risk-adapted therapeutic decisions, advancing precision oncology in neuro-oncology practice.
期刊介绍:
Cancer Management and Research is an international, peer reviewed, open access journal focusing on cancer research and the optimal use of preventative and integrated treatment interventions to achieve improved outcomes, enhanced survival, and quality of life for cancer patients. Specific topics covered in the journal include:
◦Epidemiology, detection and screening
◦Cellular research and biomarkers
◦Identification of biotargets and agents with novel mechanisms of action
◦Optimal clinical use of existing anticancer agents, including combination therapies
◦Radiation and surgery
◦Palliative care
◦Patient adherence, quality of life, satisfaction
The journal welcomes submitted papers covering original research, basic science, clinical & epidemiological studies, reviews & evaluations, guidelines, expert opinion and commentary, and case series that shed novel insights on a disease or disease subtype.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


