Hamad J AlBassam, Wael Alanazi, Faisal Al Rashid, Zainab I Alruwaii, Zainab Almusa
{"title":"侵袭性胃肠道毛霉菌病表现为中性粒细胞减少性小肠结肠炎1例。","authors":"Hamad J AlBassam, Wael Alanazi, Faisal Al Rashid, Zainab I Alruwaii, Zainab Almusa","doi":"10.12659/AJCR.948878","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Gastrointestinal mucormycosis is an underrecognized and underreported fungal infection with a high mortality rate. Diagnosis is often confounded by a non-specific constellation of signs and symptoms. We present a case of neutropenic colitis and ileocecal perforation secondary to gastrointestinal mucormycosis. CASE REPORT The patient was a 19-year-old man recently diagnosed with B-cell acute lymphoblastic leukemia, on active chemotherapy. He presented with abdominal pain and tenderness, and a contrast-enhanced CT revealed neutropenic colitis. Despite broad-spectrum antibiotics, his condition worsened, prompting reassessment. Follow-up CT showed bowel ischemia and a pelvic collection. He underwent an emergency laparotomy, which revealed destruction of the anterior cecal wall and detachment from the terminal ileum and ascending colon. Ileocecal resection was performed and histopathologic examination demonstrated angioinvasive fungal elements consistent with Mucor spp. He was diagnosed with gastrointestinal mucormycosis and promptly started on amphotericin intravenously. He improved over the next 2 weeks and was discharged with a plan to continue his 6-week course as an outpatient, followed by oral posaconazole maintenance therapy. Several weeks later, his infection relapsed secondary to non-compliance. He underwent repeat surgical debridement and antimicrobial therapy was restarted with intravenous amphotericin and Isavuconazole. He successfully completed 6 weeks of treatment and was transitioned to oral Isavuconazole prophylaxis. He remained stable and relapse-free at 6 months following his second procedure. CONCLUSIONS The case highlights the importance of early recognition of patients at risk for this infection, maintaining a high index of suspicion, and employing aggressive medical and surgical management strategies to avoid mortality.</p>","PeriodicalId":39064,"journal":{"name":"American Journal of Case Reports","volume":"26 ","pages":"e948878"},"PeriodicalIF":0.7000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12427590/pdf/","citationCount":"0","resultStr":"{\"title\":\"Invasive Gastrointestinal Mucormycosis Presenting as Neutropenic Enterocolitis: A Case Report.\",\"authors\":\"Hamad J AlBassam, Wael Alanazi, Faisal Al Rashid, Zainab I Alruwaii, Zainab Almusa\",\"doi\":\"10.12659/AJCR.948878\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BACKGROUND Gastrointestinal mucormycosis is an underrecognized and underreported fungal infection with a high mortality rate. Diagnosis is often confounded by a non-specific constellation of signs and symptoms. We present a case of neutropenic colitis and ileocecal perforation secondary to gastrointestinal mucormycosis. CASE REPORT The patient was a 19-year-old man recently diagnosed with B-cell acute lymphoblastic leukemia, on active chemotherapy. He presented with abdominal pain and tenderness, and a contrast-enhanced CT revealed neutropenic colitis. Despite broad-spectrum antibiotics, his condition worsened, prompting reassessment. Follow-up CT showed bowel ischemia and a pelvic collection. He underwent an emergency laparotomy, which revealed destruction of the anterior cecal wall and detachment from the terminal ileum and ascending colon. Ileocecal resection was performed and histopathologic examination demonstrated angioinvasive fungal elements consistent with Mucor spp. He was diagnosed with gastrointestinal mucormycosis and promptly started on amphotericin intravenously. He improved over the next 2 weeks and was discharged with a plan to continue his 6-week course as an outpatient, followed by oral posaconazole maintenance therapy. Several weeks later, his infection relapsed secondary to non-compliance. He underwent repeat surgical debridement and antimicrobial therapy was restarted with intravenous amphotericin and Isavuconazole. He successfully completed 6 weeks of treatment and was transitioned to oral Isavuconazole prophylaxis. He remained stable and relapse-free at 6 months following his second procedure. CONCLUSIONS The case highlights the importance of early recognition of patients at risk for this infection, maintaining a high index of suspicion, and employing aggressive medical and surgical management strategies to avoid mortality.</p>\",\"PeriodicalId\":39064,\"journal\":{\"name\":\"American Journal of Case Reports\",\"volume\":\"26 \",\"pages\":\"e948878\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12427590/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12659/AJCR.948878\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.948878","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Invasive Gastrointestinal Mucormycosis Presenting as Neutropenic Enterocolitis: A Case Report.
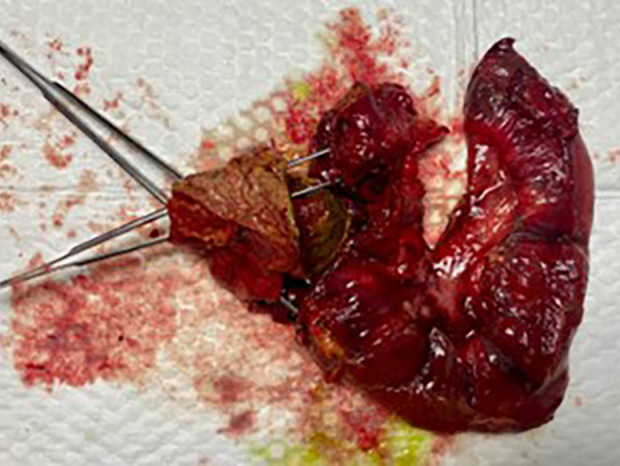
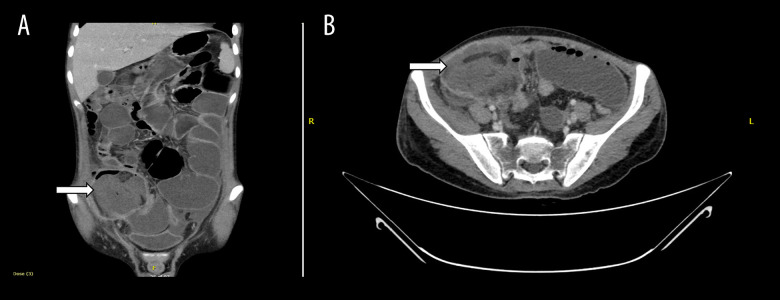
BACKGROUND Gastrointestinal mucormycosis is an underrecognized and underreported fungal infection with a high mortality rate. Diagnosis is often confounded by a non-specific constellation of signs and symptoms. We present a case of neutropenic colitis and ileocecal perforation secondary to gastrointestinal mucormycosis. CASE REPORT The patient was a 19-year-old man recently diagnosed with B-cell acute lymphoblastic leukemia, on active chemotherapy. He presented with abdominal pain and tenderness, and a contrast-enhanced CT revealed neutropenic colitis. Despite broad-spectrum antibiotics, his condition worsened, prompting reassessment. Follow-up CT showed bowel ischemia and a pelvic collection. He underwent an emergency laparotomy, which revealed destruction of the anterior cecal wall and detachment from the terminal ileum and ascending colon. Ileocecal resection was performed and histopathologic examination demonstrated angioinvasive fungal elements consistent with Mucor spp. He was diagnosed with gastrointestinal mucormycosis and promptly started on amphotericin intravenously. He improved over the next 2 weeks and was discharged with a plan to continue his 6-week course as an outpatient, followed by oral posaconazole maintenance therapy. Several weeks later, his infection relapsed secondary to non-compliance. He underwent repeat surgical debridement and antimicrobial therapy was restarted with intravenous amphotericin and Isavuconazole. He successfully completed 6 weeks of treatment and was transitioned to oral Isavuconazole prophylaxis. He remained stable and relapse-free at 6 months following his second procedure. CONCLUSIONS The case highlights the importance of early recognition of patients at risk for this infection, maintaining a high index of suspicion, and employing aggressive medical and surgical management strategies to avoid mortality.
期刊介绍:
American Journal of Case Reports is an international, peer-reviewed scientific journal that publishes single and series case reports in all medical fields. American Journal of Case Reports is issued on a continuous basis as a primary electronic journal. Print copies of a single article or a set of articles can be ordered on demand.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


