Justin Engelbrecht, Chandbi Tajeer, Cara O'Connor, Kate Rees
{"title":"差异化抗逆转录病毒分发:在南非五个地区实施。","authors":"Justin Engelbrecht, Chandbi Tajeer, Cara O'Connor, Kate Rees","doi":"10.4102/phcfm.v17i1.4974","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong> The National Department of Health introduced Differentiated Service Delivery (DSD) models to improve retention in care and decongest healthcare facilities. Anova Health Institute supported the implementation of DSD guidelines in five districts of South Africa.</p><p><strong>Aim: </strong> The study aimed to describe how the models contained in DSD policies are operationalised.</p><p><strong>Setting: </strong> Five districts of South Africa - two metropolitan, two mixed and one rural.</p><p><strong>Methods: </strong> We used a mixed-methods approach, incorporating a 2-day participatory workshop in 2023 and a retrospective review of routine programmatic data. A mapping exercise was used to understand all models of chronic medication provision in the five study districts and to describe differences in operationalisation. We also report on the number of options per facility and healthcare provider perspectives of benefits and limitations.</p><p><strong>Results: </strong> External and facility pick-up points were the most commonly implemented models. Three key themes were: the trade-off between convenience and additional support, the trade-off between controlling client care and outsourcing tasks and the distribution of work between cadres of staff. Sedibeng District provided the most options per facility, with 57% of facilities having three possible options. Cape Town provided the fewest, with 50% of facilities offering only one option.</p><p><strong>Conclusion: </strong> Health and environmental contexts guide the choice of DSD modalities offered. It is possible to offer clients options in South African settings.Contribution: This study highlights the context-specific nature of DSD model implementation and the importance of client choice. Further research into availability and options from a client perspective would be useful.</p>","PeriodicalId":47037,"journal":{"name":"African Journal of Primary Health Care & Family Medicine","volume":"17 1","pages":"e1-e9"},"PeriodicalIF":1.7000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421779/pdf/","citationCount":"0","resultStr":"{\"title\":\"Differentiated antiretroviral distribution: Implementation in five South African districts.\",\"authors\":\"Justin Engelbrecht, Chandbi Tajeer, Cara O'Connor, Kate Rees\",\"doi\":\"10.4102/phcfm.v17i1.4974\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong> The National Department of Health introduced Differentiated Service Delivery (DSD) models to improve retention in care and decongest healthcare facilities. Anova Health Institute supported the implementation of DSD guidelines in five districts of South Africa.</p><p><strong>Aim: </strong> The study aimed to describe how the models contained in DSD policies are operationalised.</p><p><strong>Setting: </strong> Five districts of South Africa - two metropolitan, two mixed and one rural.</p><p><strong>Methods: </strong> We used a mixed-methods approach, incorporating a 2-day participatory workshop in 2023 and a retrospective review of routine programmatic data. A mapping exercise was used to understand all models of chronic medication provision in the five study districts and to describe differences in operationalisation. We also report on the number of options per facility and healthcare provider perspectives of benefits and limitations.</p><p><strong>Results: </strong> External and facility pick-up points were the most commonly implemented models. Three key themes were: the trade-off between convenience and additional support, the trade-off between controlling client care and outsourcing tasks and the distribution of work between cadres of staff. Sedibeng District provided the most options per facility, with 57% of facilities having three possible options. Cape Town provided the fewest, with 50% of facilities offering only one option.</p><p><strong>Conclusion: </strong> Health and environmental contexts guide the choice of DSD modalities offered. It is possible to offer clients options in South African settings.Contribution: This study highlights the context-specific nature of DSD model implementation and the importance of client choice. Further research into availability and options from a client perspective would be useful.</p>\",\"PeriodicalId\":47037,\"journal\":{\"name\":\"African Journal of Primary Health Care & Family Medicine\",\"volume\":\"17 1\",\"pages\":\"e1-e9\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421779/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"African Journal of Primary Health Care & Family Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4102/phcfm.v17i1.4974\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q4\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"African Journal of Primary Health Care & Family Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4102/phcfm.v17i1.4974","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
Differentiated antiretroviral distribution: Implementation in five South African districts.
Background: The National Department of Health introduced Differentiated Service Delivery (DSD) models to improve retention in care and decongest healthcare facilities. Anova Health Institute supported the implementation of DSD guidelines in five districts of South Africa.
Aim: The study aimed to describe how the models contained in DSD policies are operationalised.
Setting: Five districts of South Africa - two metropolitan, two mixed and one rural.
Methods: We used a mixed-methods approach, incorporating a 2-day participatory workshop in 2023 and a retrospective review of routine programmatic data. A mapping exercise was used to understand all models of chronic medication provision in the five study districts and to describe differences in operationalisation. We also report on the number of options per facility and healthcare provider perspectives of benefits and limitations.
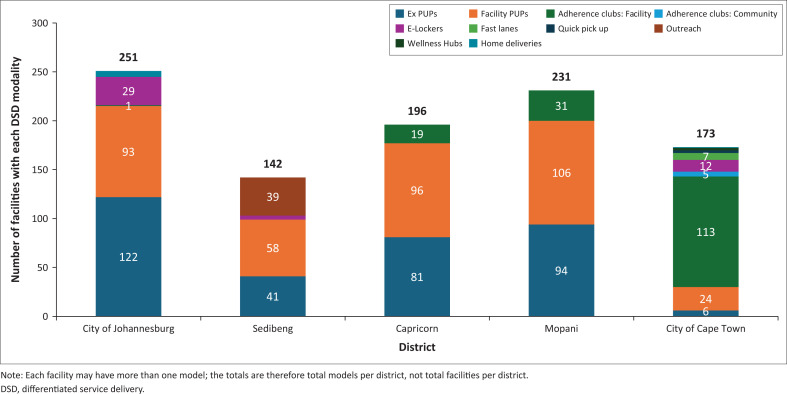
Results: External and facility pick-up points were the most commonly implemented models. Three key themes were: the trade-off between convenience and additional support, the trade-off between controlling client care and outsourcing tasks and the distribution of work between cadres of staff. Sedibeng District provided the most options per facility, with 57% of facilities having three possible options. Cape Town provided the fewest, with 50% of facilities offering only one option.
Conclusion: Health and environmental contexts guide the choice of DSD modalities offered. It is possible to offer clients options in South African settings.Contribution: This study highlights the context-specific nature of DSD model implementation and the importance of client choice. Further research into availability and options from a client perspective would be useful.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


