{"title":"多囊性肝病肝移植术中形成气膨出:成功的非手术治疗。","authors":"Satoshi Takada, Shinichi Nakanuma, Renta Kobori, Takahiro Araki, Kazuki Kato, Abdulrahman Nasr, Ryohei Takei, Daisuke Saito, Kaichiro Kato, Mitsuyoshi Okazaki, Isamu Makino, Shintaro Yagi","doi":"10.70352/scrj.cr.25-0341","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Liver transplantation for polycystic liver disease (PLD) poses significant intraoperative risks due to the presence of a massively enlarged liver. We report a rare case of intraoperative pneumothorax and pneumatocele formation during total hepatectomy, which was successfully managed with a non-operative approach.</p><p><strong>Case presentation: </strong>A female patient in her 40s with a history of autosomal dominant polycystic kidney disease presented with progressive liver cyst enlargement (Gigot type III, Qian classification Grade 4), which led to decreased activities of daily living and intracystic hemorrhage. The patient underwent a deceased-donor liver transplantation. During mobilization of the liver from the right side of the diaphragm, the patient experienced sudden onset of pneumothorax. Incision of the diaphragm revealed a cystic structure containing a hematoma, suggesting pneumatocele formation. The pneumatocele was not resected during the ongoing operation; instead, thoracic drainage was performed as the primary intervention. Postoperatively, no air leakage was observed, and the thoracic drain was successfully removed on POD 12. The pneumatocele, which measured approximately 10 × 10 × 7 cm, showed no signs of infection, and was monitored without additional surgical intervention. On POD 19, a fever prompted further evaluation, and CT-guided cyst aspiration for culture was performed, which revealed no evidence of infection. Acute T-cell-mediated rejection was observed on POD 27, and a steroid pulse was administered, but even after that, the pneumatocele gradually decreased in size without any signs of infection.</p><p><strong>Conclusions: </strong>A pneumatocele is an uncommon but important consideration during liver transplantation for PLD, potentially resulting from barotrauma related to abrupt changes in intrathoracic pressure during hepatectomy and mechanical ventilation. Considering the risk of infection in immunosuppressed patients, close monitoring is essential. On the contrary, surgical resection also carries the risk of pulmonary or bronchial fistulae; therefore, careful consideration is required. This case demonstrates that non-operative management with careful observation can be an effective strategy in selected patients.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414612/pdf/","citationCount":"0","resultStr":"{\"title\":\"Intraoperative Pneumatocele Formation during Liver Transplantation for Polycystic Liver Disease: Successful Non-Operative Management.\",\"authors\":\"Satoshi Takada, Shinichi Nakanuma, Renta Kobori, Takahiro Araki, Kazuki Kato, Abdulrahman Nasr, Ryohei Takei, Daisuke Saito, Kaichiro Kato, Mitsuyoshi Okazaki, Isamu Makino, Shintaro Yagi\",\"doi\":\"10.70352/scrj.cr.25-0341\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Liver transplantation for polycystic liver disease (PLD) poses significant intraoperative risks due to the presence of a massively enlarged liver. We report a rare case of intraoperative pneumothorax and pneumatocele formation during total hepatectomy, which was successfully managed with a non-operative approach.</p><p><strong>Case presentation: </strong>A female patient in her 40s with a history of autosomal dominant polycystic kidney disease presented with progressive liver cyst enlargement (Gigot type III, Qian classification Grade 4), which led to decreased activities of daily living and intracystic hemorrhage. The patient underwent a deceased-donor liver transplantation. During mobilization of the liver from the right side of the diaphragm, the patient experienced sudden onset of pneumothorax. Incision of the diaphragm revealed a cystic structure containing a hematoma, suggesting pneumatocele formation. The pneumatocele was not resected during the ongoing operation; instead, thoracic drainage was performed as the primary intervention. Postoperatively, no air leakage was observed, and the thoracic drain was successfully removed on POD 12. The pneumatocele, which measured approximately 10 × 10 × 7 cm, showed no signs of infection, and was monitored without additional surgical intervention. On POD 19, a fever prompted further evaluation, and CT-guided cyst aspiration for culture was performed, which revealed no evidence of infection. Acute T-cell-mediated rejection was observed on POD 27, and a steroid pulse was administered, but even after that, the pneumatocele gradually decreased in size without any signs of infection.</p><p><strong>Conclusions: </strong>A pneumatocele is an uncommon but important consideration during liver transplantation for PLD, potentially resulting from barotrauma related to abrupt changes in intrathoracic pressure during hepatectomy and mechanical ventilation. Considering the risk of infection in immunosuppressed patients, close monitoring is essential. On the contrary, surgical resection also carries the risk of pulmonary or bronchial fistulae; therefore, careful consideration is required. This case demonstrates that non-operative management with careful observation can be an effective strategy in selected patients.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414612/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.25-0341\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/2 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0341","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/2 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Intraoperative Pneumatocele Formation during Liver Transplantation for Polycystic Liver Disease: Successful Non-Operative Management.
Introduction: Liver transplantation for polycystic liver disease (PLD) poses significant intraoperative risks due to the presence of a massively enlarged liver. We report a rare case of intraoperative pneumothorax and pneumatocele formation during total hepatectomy, which was successfully managed with a non-operative approach.
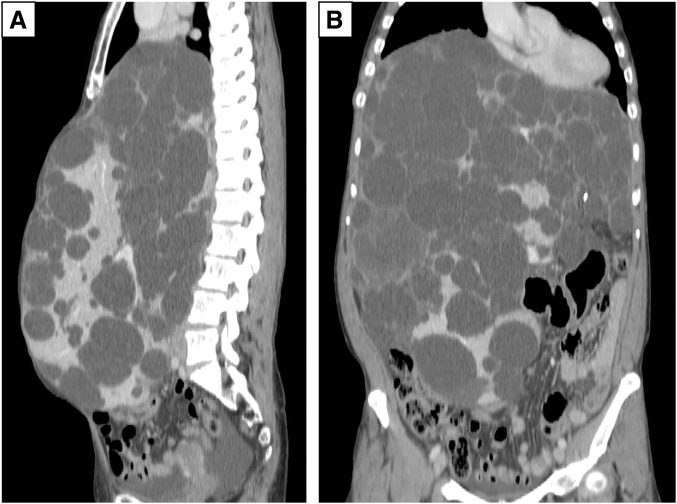
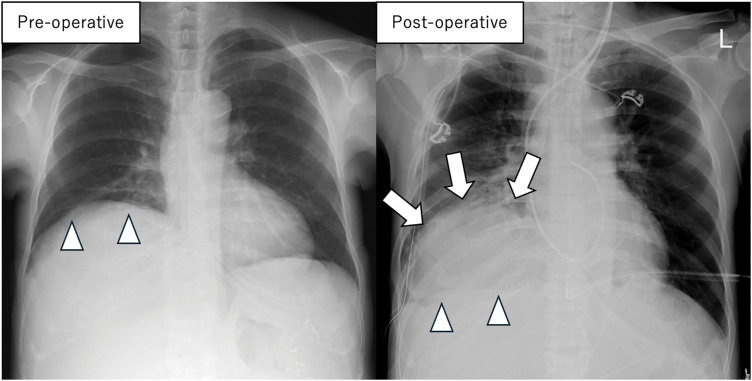
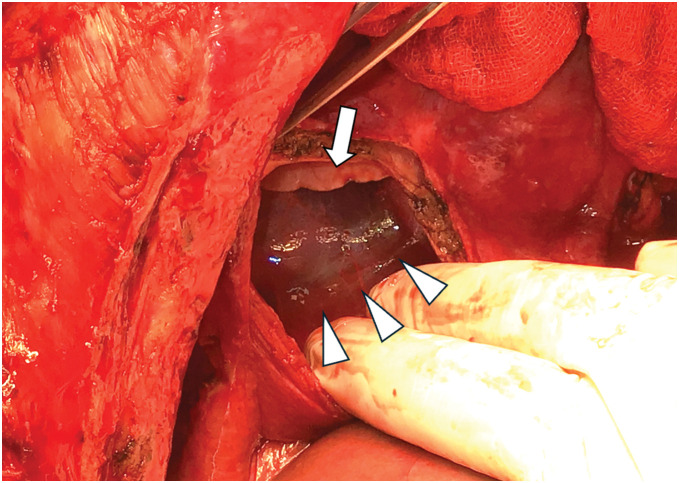
Case presentation: A female patient in her 40s with a history of autosomal dominant polycystic kidney disease presented with progressive liver cyst enlargement (Gigot type III, Qian classification Grade 4), which led to decreased activities of daily living and intracystic hemorrhage. The patient underwent a deceased-donor liver transplantation. During mobilization of the liver from the right side of the diaphragm, the patient experienced sudden onset of pneumothorax. Incision of the diaphragm revealed a cystic structure containing a hematoma, suggesting pneumatocele formation. The pneumatocele was not resected during the ongoing operation; instead, thoracic drainage was performed as the primary intervention. Postoperatively, no air leakage was observed, and the thoracic drain was successfully removed on POD 12. The pneumatocele, which measured approximately 10 × 10 × 7 cm, showed no signs of infection, and was monitored without additional surgical intervention. On POD 19, a fever prompted further evaluation, and CT-guided cyst aspiration for culture was performed, which revealed no evidence of infection. Acute T-cell-mediated rejection was observed on POD 27, and a steroid pulse was administered, but even after that, the pneumatocele gradually decreased in size without any signs of infection.
Conclusions: A pneumatocele is an uncommon but important consideration during liver transplantation for PLD, potentially resulting from barotrauma related to abrupt changes in intrathoracic pressure during hepatectomy and mechanical ventilation. Considering the risk of infection in immunosuppressed patients, close monitoring is essential. On the contrary, surgical resection also carries the risk of pulmonary or bronchial fistulae; therefore, careful consideration is required. This case demonstrates that non-operative management with careful observation can be an effective strategy in selected patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


