{"title":"10价肺炎球菌结合疫苗(PCV10)和PPSV23序贯接种对系统性红斑狼疮的免疫原性、安全性和不良事件与单独接种PPSV23的比较","authors":"Rudrarpan Chatterjee, Sai Yasaswini Kommaraju, Shincy Mettingal Ramakrishnan, Kadahalli Lingegowda Ravikumar, Amita Aggarwal","doi":"10.1136/lupus-2025-001551","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>SLE has increased risk of invasive pneumococcal disease due to immune dysregulation and immunosuppression. European Alliance of Associations for Rheumatology recommendations suggest sequential vaccination with conjugate vaccine, followed by 23-valent pneumococcal polysaccharide vaccine (PPSV23). However, data on immunogenicity of sequential vaccination in SLE are limited.</p><p><strong>Methods: </strong>Adult patients with SLE (American College of Rheumatology 2019 criteria) with inactive disease, stable immunosuppression for 3 months and prednisolone ≤10 mg/day were included. Sequential arm received 10-valent pneumococcal conjugate vaccine, followed by PPSV23. The second arm received only PPSV23. The two cohorts were recruited independently without randomisation. Antibodies at baseline and 12-14 weeks to pneumococci (serotypes 1, 5, 6B, 14 and 19F) were measured by ELISA and opsonophagocytic assay for functional antibodies. The primary outcome was a twofold increase in 3/5 serotypes. 40 subjects were enrolled in each arm and 15 healthy adults for response to PPSV23.</p><p><strong>Results: </strong>35 completed the study in the PPSV23 arm and 34 in the sequential arm. Baseline parameters were comparable.Response to PPSV23 was poorer in SLE (74.28%) compared with healthy controls (100%). There was no difference in the primary outcome between sequential vaccination (82.35%, 95% CI 68% to 94%) and PPSV23 (74.28%, 95% CI 60% to 89%). All 15 non-responders were on prednisolone. Among responders, only 41/54 (76%) were on prednisolone. There was no difference in other immunosuppressive drugs. Increasing age predicted poor response on multivariable analysis in all serotypes.Major adverse events included one event of Miller Fisher variant of Guillain-Barré syndrome in the sequential arm. Minor adverse events included one each with injection-site pain, migraine, fever and fatigue after conjugate vaccine, and one with fever after PPSV23. Three minor adverse events in the PPSV23 group included one each with injection-site pain, <i>herpes zoster</i>, headache and fever. In the PPSV23 arm, three minor flares were seen, while in the sequential arm, one major flare and one minor flare occurred.</p><p><strong>Interpretation: </strong>Both vaccination strategies are safe with adequate antibody response. In low- and middle-income countries, a single-dose PPSV23 may be adequate if cost negates sequential vaccination.</p>","PeriodicalId":18126,"journal":{"name":"Lupus Science & Medicine","volume":"12 2","pages":""},"PeriodicalIF":3.5000,"publicationDate":"2025-09-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421157/pdf/","citationCount":"0","resultStr":"{\"title\":\"Immunogenicity, safety and adverse events of sequential vaccination with a 10-valent pneumococcal conjugate vaccine (PCV10) and PPSV23 compared with PPSV23 alone in systemic lupus erythematosus.\",\"authors\":\"Rudrarpan Chatterjee, Sai Yasaswini Kommaraju, Shincy Mettingal Ramakrishnan, Kadahalli Lingegowda Ravikumar, Amita Aggarwal\",\"doi\":\"10.1136/lupus-2025-001551\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>SLE has increased risk of invasive pneumococcal disease due to immune dysregulation and immunosuppression. European Alliance of Associations for Rheumatology recommendations suggest sequential vaccination with conjugate vaccine, followed by 23-valent pneumococcal polysaccharide vaccine (PPSV23). However, data on immunogenicity of sequential vaccination in SLE are limited.</p><p><strong>Methods: </strong>Adult patients with SLE (American College of Rheumatology 2019 criteria) with inactive disease, stable immunosuppression for 3 months and prednisolone ≤10 mg/day were included. Sequential arm received 10-valent pneumococcal conjugate vaccine, followed by PPSV23. The second arm received only PPSV23. The two cohorts were recruited independently without randomisation. Antibodies at baseline and 12-14 weeks to pneumococci (serotypes 1, 5, 6B, 14 and 19F) were measured by ELISA and opsonophagocytic assay for functional antibodies. The primary outcome was a twofold increase in 3/5 serotypes. 40 subjects were enrolled in each arm and 15 healthy adults for response to PPSV23.</p><p><strong>Results: </strong>35 completed the study in the PPSV23 arm and 34 in the sequential arm. Baseline parameters were comparable.Response to PPSV23 was poorer in SLE (74.28%) compared with healthy controls (100%). There was no difference in the primary outcome between sequential vaccination (82.35%, 95% CI 68% to 94%) and PPSV23 (74.28%, 95% CI 60% to 89%). All 15 non-responders were on prednisolone. Among responders, only 41/54 (76%) were on prednisolone. There was no difference in other immunosuppressive drugs. Increasing age predicted poor response on multivariable analysis in all serotypes.Major adverse events included one event of Miller Fisher variant of Guillain-Barré syndrome in the sequential arm. Minor adverse events included one each with injection-site pain, migraine, fever and fatigue after conjugate vaccine, and one with fever after PPSV23. Three minor adverse events in the PPSV23 group included one each with injection-site pain, <i>herpes zoster</i>, headache and fever. In the PPSV23 arm, three minor flares were seen, while in the sequential arm, one major flare and one minor flare occurred.</p><p><strong>Interpretation: </strong>Both vaccination strategies are safe with adequate antibody response. In low- and middle-income countries, a single-dose PPSV23 may be adequate if cost negates sequential vaccination.</p>\",\"PeriodicalId\":18126,\"journal\":{\"name\":\"Lupus Science & Medicine\",\"volume\":\"12 2\",\"pages\":\"\"},\"PeriodicalIF\":3.5000,\"publicationDate\":\"2025-09-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12421157/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Lupus Science & Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1136/lupus-2025-001551\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RHEUMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Lupus Science & Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/lupus-2025-001551","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RHEUMATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:SLE由于免疫失调和免疫抑制而增加了侵袭性肺炎球菌疾病的风险。欧洲风湿病协会联盟建议依次接种结合疫苗,然后接种23价肺炎球菌多糖疫苗(PPSV23)。然而,关于顺序接种SLE疫苗的免疫原性的数据是有限的。方法:纳入疾病不活跃、免疫抑制稳定3个月、强的松龙≤10 mg/天的SLE成年患者(美国风湿病学会2019年标准)。顺序组接种10价肺炎球菌结合疫苗,随后接种PPSV23。第二组只接受了PPSV23。这两个队列是独立招募的,没有随机分组。在基线和12-14周时,采用ELISA和功能抗体调节噬细胞法检测肺炎球菌抗体(血清型1、5、6B、14和19F)。主要结果是3/5血清型增加了两倍。每组40名受试者和15名健康成人对PPSV23的反应。结果:PPSV23组35人完成研究,序贯组34人完成研究。基线参数具有可比性。与健康对照组(100%)相比,SLE患者对PPSV23的反应较差(74.28%)。序次接种(82.35%,95% CI 68% - 94%)和PPSV23 (74.28%, 95% CI 60% - 89%)的主要结局无差异。所有15名无反应者均接受泼尼松龙治疗。在应答者中,只有41/54(76%)使用强的松龙。其他免疫抑制药物无差异。在所有血清型的多变量分析中,年龄的增加预示着不良反应。主要不良事件包括顺序组中一例米勒-费雪变异格林-巴罗综合征。轻微不良事件包括接种结合疫苗后出现注射部位疼痛、偏头痛、发热和疲劳各1例,接种PPSV23后出现发热1例。PPSV23组的三个轻微不良事件包括注射部位疼痛、带状疱疹、头痛和发烧。在PPSV23组中,观察到三次轻微耀斑,而在顺序组中,发生了一次主要耀斑和一次次要耀斑。解释:两种疫苗接种策略都是安全的,有足够的抗体反应。在低收入和中等收入国家,如果费用不允许连续接种疫苗,单剂PPSV23可能就足够了。
Immunogenicity, safety and adverse events of sequential vaccination with a 10-valent pneumococcal conjugate vaccine (PCV10) and PPSV23 compared with PPSV23 alone in systemic lupus erythematosus.
Background: SLE has increased risk of invasive pneumococcal disease due to immune dysregulation and immunosuppression. European Alliance of Associations for Rheumatology recommendations suggest sequential vaccination with conjugate vaccine, followed by 23-valent pneumococcal polysaccharide vaccine (PPSV23). However, data on immunogenicity of sequential vaccination in SLE are limited.
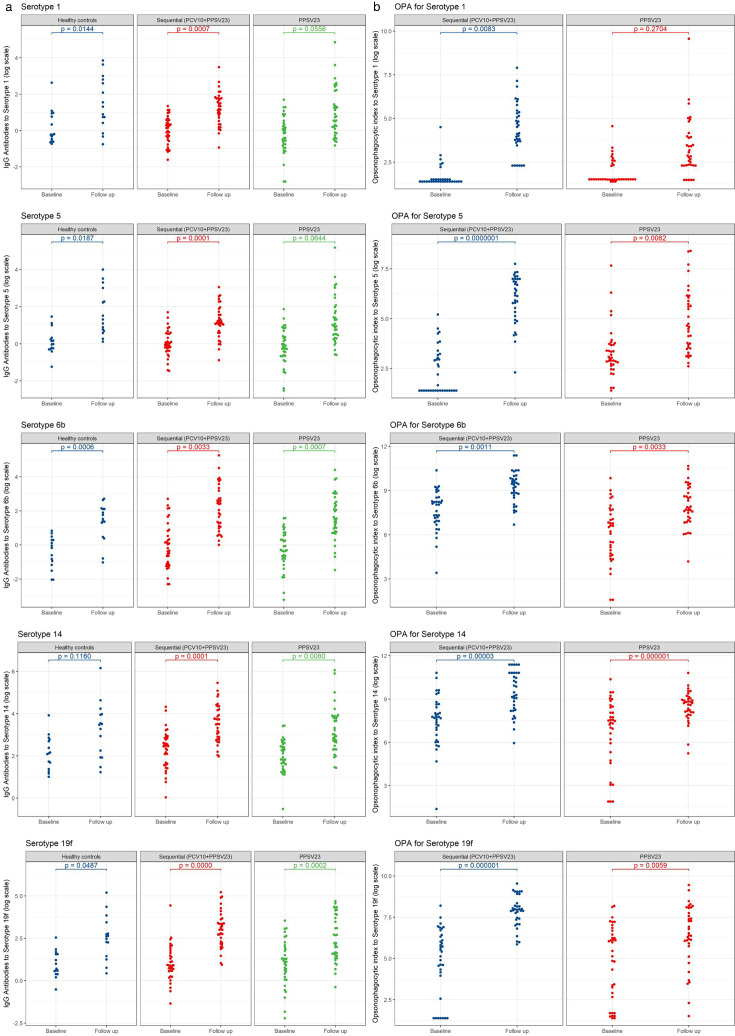
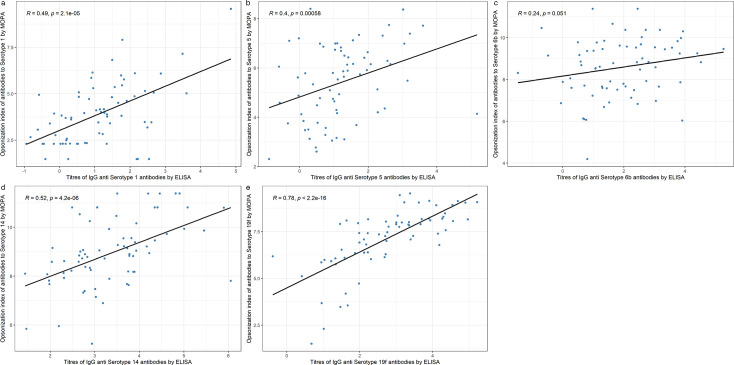
Methods: Adult patients with SLE (American College of Rheumatology 2019 criteria) with inactive disease, stable immunosuppression for 3 months and prednisolone ≤10 mg/day were included. Sequential arm received 10-valent pneumococcal conjugate vaccine, followed by PPSV23. The second arm received only PPSV23. The two cohorts were recruited independently without randomisation. Antibodies at baseline and 12-14 weeks to pneumococci (serotypes 1, 5, 6B, 14 and 19F) were measured by ELISA and opsonophagocytic assay for functional antibodies. The primary outcome was a twofold increase in 3/5 serotypes. 40 subjects were enrolled in each arm and 15 healthy adults for response to PPSV23.
Results: 35 completed the study in the PPSV23 arm and 34 in the sequential arm. Baseline parameters were comparable.Response to PPSV23 was poorer in SLE (74.28%) compared with healthy controls (100%). There was no difference in the primary outcome between sequential vaccination (82.35%, 95% CI 68% to 94%) and PPSV23 (74.28%, 95% CI 60% to 89%). All 15 non-responders were on prednisolone. Among responders, only 41/54 (76%) were on prednisolone. There was no difference in other immunosuppressive drugs. Increasing age predicted poor response on multivariable analysis in all serotypes.Major adverse events included one event of Miller Fisher variant of Guillain-Barré syndrome in the sequential arm. Minor adverse events included one each with injection-site pain, migraine, fever and fatigue after conjugate vaccine, and one with fever after PPSV23. Three minor adverse events in the PPSV23 group included one each with injection-site pain, herpes zoster, headache and fever. In the PPSV23 arm, three minor flares were seen, while in the sequential arm, one major flare and one minor flare occurred.
Interpretation: Both vaccination strategies are safe with adequate antibody response. In low- and middle-income countries, a single-dose PPSV23 may be adequate if cost negates sequential vaccination.
期刊介绍:
Lupus Science & Medicine is a global, peer reviewed, open access online journal that provides a central point for publication of basic, clinical, translational, and epidemiological studies of all aspects of lupus and related diseases. It is the first lupus-specific open access journal in the world and was developed in response to the need for a barrier-free forum for publication of groundbreaking studies in lupus. The journal publishes research on lupus from fields including, but not limited to: rheumatology, dermatology, nephrology, immunology, pediatrics, cardiology, hepatology, pulmonology, obstetrics and gynecology, and psychiatry.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


