Boohwi Hong, Yumin Jo, Sujin Baek, Woosuk Chung, Chahyun Oh, Seyeon Park
{"title":"经腹平面和腰方肌阻滞对腹腔镜肾切除术的镇痛作用无临床意义:系统综述和网络荟萃分析。","authors":"Boohwi Hong, Yumin Jo, Sujin Baek, Woosuk Chung, Chahyun Oh, Seyeon Park","doi":"10.3344/kjp.25147","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ultrasound-guided abdominal wall blocks are increasingly used to enhance postoperative analgesia in laparoscopic nephrectomy. Among these, the transversus abdominis plane (TAP) block and the quadratus lumborum (QL) block have emerged as promising techniques. However, no comprehensive review has yet compared the analgesic efficacy of these two regional approaches.</p><p><strong>Methods: </strong>An extensive search was conducted across MEDLINE, Embase, Cochrane Library, Web of Science, and Google Scholar to identify randomized controlled trials comparing the postoperative analgesic effects of the TAP block, QL block, and systemic analgesia. The primary outcome was 24-hour opioid consumption, standardized to intravenous morphine milligram equivalents (MME). Secondary outcomes included postoperative pain scores assessed using a 0-10 Visual Analog Scale (VAS). A minimal clinically important difference (MCID) was defined as a reduction of 10 mg MME or 1 point on the VAS.</p><p><strong>Results: </strong>Twelve studies were included. Both TAP and QL blocks significantly reduced opioid consumption compared to systemic analgesia (mean difference [95% confidence interval, CI]: QL, -11.42 mg [-18.88 to -3.97]; TAP, -10.88 mg [-17.49 to -4.26]). However, the 95% CI did not meet the predefined MCID of -10 mg. Similarly, improvements in postoperative pain scores did not reach clinical significance.</p><p><strong>Conclusions: </strong>While TAP and QL blocks demonstrated a significant analgesic effect compared to systemic analgesia, the clinical relevance of this benefit may be limited.</p>","PeriodicalId":56252,"journal":{"name":"Korean Journal of Pain","volume":" ","pages":"412-426"},"PeriodicalIF":3.1000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12485473/pdf/","citationCount":"0","resultStr":"{\"title\":\"Analgesic effects of transversus abdominis plane and quadratus lumborum blocks are not clinically meaningful for laparoscopic nephrectomy: systematic review and network meta-analysis.\",\"authors\":\"Boohwi Hong, Yumin Jo, Sujin Baek, Woosuk Chung, Chahyun Oh, Seyeon Park\",\"doi\":\"10.3344/kjp.25147\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Ultrasound-guided abdominal wall blocks are increasingly used to enhance postoperative analgesia in laparoscopic nephrectomy. Among these, the transversus abdominis plane (TAP) block and the quadratus lumborum (QL) block have emerged as promising techniques. However, no comprehensive review has yet compared the analgesic efficacy of these two regional approaches.</p><p><strong>Methods: </strong>An extensive search was conducted across MEDLINE, Embase, Cochrane Library, Web of Science, and Google Scholar to identify randomized controlled trials comparing the postoperative analgesic effects of the TAP block, QL block, and systemic analgesia. The primary outcome was 24-hour opioid consumption, standardized to intravenous morphine milligram equivalents (MME). Secondary outcomes included postoperative pain scores assessed using a 0-10 Visual Analog Scale (VAS). A minimal clinically important difference (MCID) was defined as a reduction of 10 mg MME or 1 point on the VAS.</p><p><strong>Results: </strong>Twelve studies were included. Both TAP and QL blocks significantly reduced opioid consumption compared to systemic analgesia (mean difference [95% confidence interval, CI]: QL, -11.42 mg [-18.88 to -3.97]; TAP, -10.88 mg [-17.49 to -4.26]). However, the 95% CI did not meet the predefined MCID of -10 mg. Similarly, improvements in postoperative pain scores did not reach clinical significance.</p><p><strong>Conclusions: </strong>While TAP and QL blocks demonstrated a significant analgesic effect compared to systemic analgesia, the clinical relevance of this benefit may be limited.</p>\",\"PeriodicalId\":56252,\"journal\":{\"name\":\"Korean Journal of Pain\",\"volume\":\" \",\"pages\":\"412-426\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12485473/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Pain\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3344/kjp.25147\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/8 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Pain","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3344/kjp.25147","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/8 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Analgesic effects of transversus abdominis plane and quadratus lumborum blocks are not clinically meaningful for laparoscopic nephrectomy: systematic review and network meta-analysis.
Background: Ultrasound-guided abdominal wall blocks are increasingly used to enhance postoperative analgesia in laparoscopic nephrectomy. Among these, the transversus abdominis plane (TAP) block and the quadratus lumborum (QL) block have emerged as promising techniques. However, no comprehensive review has yet compared the analgesic efficacy of these two regional approaches.
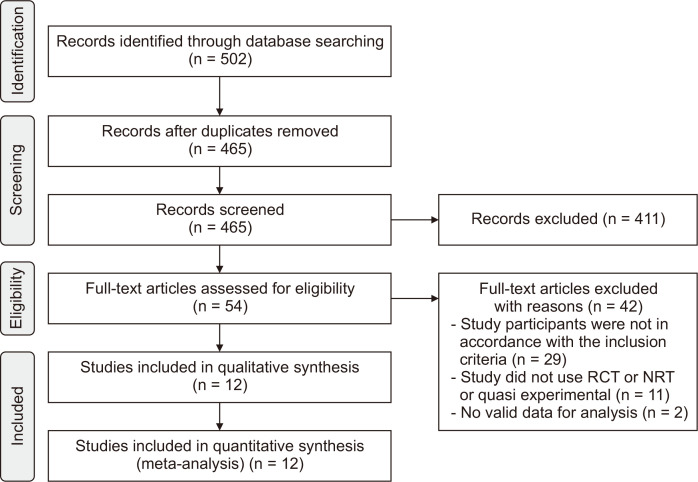
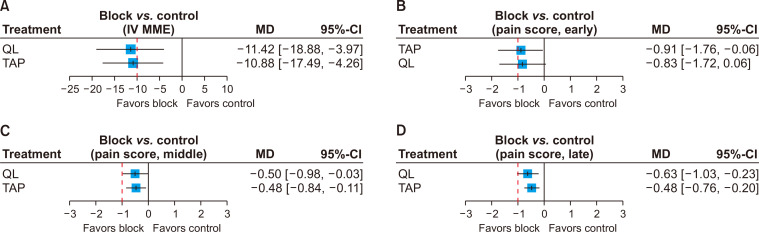
Methods: An extensive search was conducted across MEDLINE, Embase, Cochrane Library, Web of Science, and Google Scholar to identify randomized controlled trials comparing the postoperative analgesic effects of the TAP block, QL block, and systemic analgesia. The primary outcome was 24-hour opioid consumption, standardized to intravenous morphine milligram equivalents (MME). Secondary outcomes included postoperative pain scores assessed using a 0-10 Visual Analog Scale (VAS). A minimal clinically important difference (MCID) was defined as a reduction of 10 mg MME or 1 point on the VAS.
Results: Twelve studies were included. Both TAP and QL blocks significantly reduced opioid consumption compared to systemic analgesia (mean difference [95% confidence interval, CI]: QL, -11.42 mg [-18.88 to -3.97]; TAP, -10.88 mg [-17.49 to -4.26]). However, the 95% CI did not meet the predefined MCID of -10 mg. Similarly, improvements in postoperative pain scores did not reach clinical significance.
Conclusions: While TAP and QL blocks demonstrated a significant analgesic effect compared to systemic analgesia, the clinical relevance of this benefit may be limited.
期刊介绍:
Korean Journal of Pain (Korean J Pain, KJP) is the official journal of the Korean Pain Society, founded in 1986. It has been published since 1988. It publishes peer reviewed original articles related to all aspects of pain, including clinical and basic research, patient care, education, and health policy. It has been published quarterly in English since 2009 (on the first day of January, April, July, and October). In addition, it has also become the official journal of the International Spinal Pain Society since 2016. The mission of the Journal is to improve the care of patients in pain by providing a forum for clinical researchers, basic scientists, clinicians, and other health professionals. The circulation number per issue is 50.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


