Meredith Bentley, Jordan Gaal, Janice Hostetter, Suzanne Holroyd, John Pickstone, Kelly Melvin
{"title":"出现紧张性症状的迟发性后毒性脑白质病1例报告。","authors":"Meredith Bentley, Jordan Gaal, Janice Hostetter, Suzanne Holroyd, John Pickstone, Kelly Melvin","doi":"10.1155/crps/9978149","DOIUrl":null,"url":null,"abstract":"<p><p>Delayed posthypoxic leukoencephalopathy (DPHL) is a rare diagnosis that may present similarly to other more common neurological conditions, such as catatonia. While often seen with carbon-monoxide poisoning, it can also be due to anoxia due to other causes, such as drug overdose or cardiac arrest. Due to the delayed nature of its symptoms and overlap with other conditions, it can be initially misdiagnosed. We present a 50-year-old female patient with a history of depression who was found unresponsive, hypoxic, and febrile at her home for an unknown amount of time. The initial concern was for sepsis. Initial computed tomography (CT) of the head and magnetic resonance imaging (MRI) of the brain were normal. The patient had rhabdomyolysis with secondary renal failure, shock liver, and acute pancreatitis. Once medically stabilized, her cognition returned to a normal baseline. However, 10 days into her hospitalization, her mental state deteriorated, displaying symptoms of mutism, stupor, staring, decreased oral intake, and perseveration. Catatonia, secondary to a major depressive episode, was suspected. Lorazepam was titrated upward without result. Lack of response to lorazepam prompted a repeat brain MRI, revealing diffuse white matter changes in the frontal, temporal, parietal, and occipital lobes of both hemispheres. A diagnosis of DPHL was made. She was then started on carbidopa/levodopa 25/100 mg with improvement and was discharged to a rehabilitation facility.</p>","PeriodicalId":9631,"journal":{"name":"Case Reports in Psychiatry","volume":"2025 ","pages":"9978149"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413270/pdf/","citationCount":"0","resultStr":"{\"title\":\"Delayed Posthypoxic Leukoencephalopathy in a Catatonic-Appearing Patient: A Case Report.\",\"authors\":\"Meredith Bentley, Jordan Gaal, Janice Hostetter, Suzanne Holroyd, John Pickstone, Kelly Melvin\",\"doi\":\"10.1155/crps/9978149\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Delayed posthypoxic leukoencephalopathy (DPHL) is a rare diagnosis that may present similarly to other more common neurological conditions, such as catatonia. While often seen with carbon-monoxide poisoning, it can also be due to anoxia due to other causes, such as drug overdose or cardiac arrest. Due to the delayed nature of its symptoms and overlap with other conditions, it can be initially misdiagnosed. We present a 50-year-old female patient with a history of depression who was found unresponsive, hypoxic, and febrile at her home for an unknown amount of time. The initial concern was for sepsis. Initial computed tomography (CT) of the head and magnetic resonance imaging (MRI) of the brain were normal. The patient had rhabdomyolysis with secondary renal failure, shock liver, and acute pancreatitis. Once medically stabilized, her cognition returned to a normal baseline. However, 10 days into her hospitalization, her mental state deteriorated, displaying symptoms of mutism, stupor, staring, decreased oral intake, and perseveration. Catatonia, secondary to a major depressive episode, was suspected. Lorazepam was titrated upward without result. Lack of response to lorazepam prompted a repeat brain MRI, revealing diffuse white matter changes in the frontal, temporal, parietal, and occipital lobes of both hemispheres. A diagnosis of DPHL was made. She was then started on carbidopa/levodopa 25/100 mg with improvement and was discharged to a rehabilitation facility.</p>\",\"PeriodicalId\":9631,\"journal\":{\"name\":\"Case Reports in Psychiatry\",\"volume\":\"2025 \",\"pages\":\"9978149\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12413270/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Psychiatry\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/crps/9978149\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Psychiatry","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crps/9978149","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
Delayed Posthypoxic Leukoencephalopathy in a Catatonic-Appearing Patient: A Case Report.
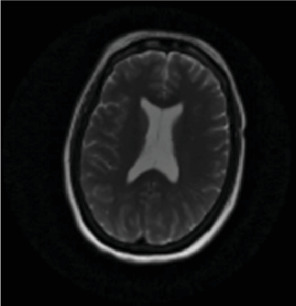
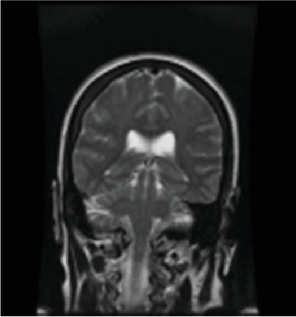
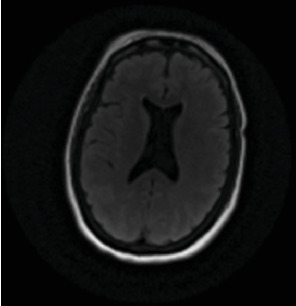
Delayed posthypoxic leukoencephalopathy (DPHL) is a rare diagnosis that may present similarly to other more common neurological conditions, such as catatonia. While often seen with carbon-monoxide poisoning, it can also be due to anoxia due to other causes, such as drug overdose or cardiac arrest. Due to the delayed nature of its symptoms and overlap with other conditions, it can be initially misdiagnosed. We present a 50-year-old female patient with a history of depression who was found unresponsive, hypoxic, and febrile at her home for an unknown amount of time. The initial concern was for sepsis. Initial computed tomography (CT) of the head and magnetic resonance imaging (MRI) of the brain were normal. The patient had rhabdomyolysis with secondary renal failure, shock liver, and acute pancreatitis. Once medically stabilized, her cognition returned to a normal baseline. However, 10 days into her hospitalization, her mental state deteriorated, displaying symptoms of mutism, stupor, staring, decreased oral intake, and perseveration. Catatonia, secondary to a major depressive episode, was suspected. Lorazepam was titrated upward without result. Lack of response to lorazepam prompted a repeat brain MRI, revealing diffuse white matter changes in the frontal, temporal, parietal, and occipital lobes of both hemispheres. A diagnosis of DPHL was made. She was then started on carbidopa/levodopa 25/100 mg with improvement and was discharged to a rehabilitation facility.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


