{"title":"通过ECHO+模式提高心血管疾病管理的初级保健能力:西弗吉尼亚州、阿肯色州和俄克拉荷马州的多州农村合作","authors":"Dru Ricci, Hannah Schmitt, Heidi Ngov, Tessa Collins, Amie Pollack, Kirsten Meisinger, Anne-Marie Anagnostopoulos, Adam Vascellaro, Brody Eaton, Janie Knotts, David Duong","doi":"10.1177/21501319251367831","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cardiovascular diseases (CVD) are the leading cause of mortality in Arkansas, West Virginia, and Oklahoma, underscoring the need for approaches to build primary care capacity to address CVD in these states.</p><p><strong>Methods: </strong>The \"ECHO+\" model integrates a CVD-focused tele-education course with quality improvement (QI) training and coaching to empower rural primary care providers (PCPs) in diagnosing and managing CVD effectively.</p><p><strong>Results: </strong>41 clinicians participated in the program. 100% reported high satisfaction and intention to apply learnings in practice. CVD knowledge and confidence increased among participants immediately post-course, with sustained improvements at a 6-month follow-up. QI teams achieved measurable improvements in clinical metrics and evidence-based CVD care practices through Plan-Do-Study-Act (PDSA) cycles, including an increase in optimized statin therapy rates from 72% to 86%. The clinical course also increased statin prescribing, with participating providers prescribing significantly more statins in the 6 months following the course than the 6 months before. Patients of participating clinicians experienced improved health outcomes, as evidenced by reductions in systolic blood pressure.</p><p><strong>Conclusion: </strong>These findings illustrate the potential of academic medical centers collaborating with rural primary care clinics to address health disparities through the ECHO+ model, which combines tele-education and QI to enhance clinician capacity and improve population health outcomes.</p>","PeriodicalId":46723,"journal":{"name":"Journal of Primary Care and Community Health","volume":"16 ","pages":"21501319251367831"},"PeriodicalIF":2.5000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414120/pdf/","citationCount":"0","resultStr":"{\"title\":\"Enhancing Primary Care Capacity for Cardiovascular Disease Management Through the ECHO+ Model: A Multistate Rural Collaboration Among West Virginia, Arkansas, and Oklahoma.\",\"authors\":\"Dru Ricci, Hannah Schmitt, Heidi Ngov, Tessa Collins, Amie Pollack, Kirsten Meisinger, Anne-Marie Anagnostopoulos, Adam Vascellaro, Brody Eaton, Janie Knotts, David Duong\",\"doi\":\"10.1177/21501319251367831\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cardiovascular diseases (CVD) are the leading cause of mortality in Arkansas, West Virginia, and Oklahoma, underscoring the need for approaches to build primary care capacity to address CVD in these states.</p><p><strong>Methods: </strong>The \\\"ECHO+\\\" model integrates a CVD-focused tele-education course with quality improvement (QI) training and coaching to empower rural primary care providers (PCPs) in diagnosing and managing CVD effectively.</p><p><strong>Results: </strong>41 clinicians participated in the program. 100% reported high satisfaction and intention to apply learnings in practice. CVD knowledge and confidence increased among participants immediately post-course, with sustained improvements at a 6-month follow-up. QI teams achieved measurable improvements in clinical metrics and evidence-based CVD care practices through Plan-Do-Study-Act (PDSA) cycles, including an increase in optimized statin therapy rates from 72% to 86%. The clinical course also increased statin prescribing, with participating providers prescribing significantly more statins in the 6 months following the course than the 6 months before. Patients of participating clinicians experienced improved health outcomes, as evidenced by reductions in systolic blood pressure.</p><p><strong>Conclusion: </strong>These findings illustrate the potential of academic medical centers collaborating with rural primary care clinics to address health disparities through the ECHO+ model, which combines tele-education and QI to enhance clinician capacity and improve population health outcomes.</p>\",\"PeriodicalId\":46723,\"journal\":{\"name\":\"Journal of Primary Care and Community Health\",\"volume\":\"16 \",\"pages\":\"21501319251367831\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12414120/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Primary Care and Community Health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/21501319251367831\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/6 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"PRIMARY HEALTH CARE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Primary Care and Community Health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/21501319251367831","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
Enhancing Primary Care Capacity for Cardiovascular Disease Management Through the ECHO+ Model: A Multistate Rural Collaboration Among West Virginia, Arkansas, and Oklahoma.
Background: Cardiovascular diseases (CVD) are the leading cause of mortality in Arkansas, West Virginia, and Oklahoma, underscoring the need for approaches to build primary care capacity to address CVD in these states.
Methods: The "ECHO+" model integrates a CVD-focused tele-education course with quality improvement (QI) training and coaching to empower rural primary care providers (PCPs) in diagnosing and managing CVD effectively.
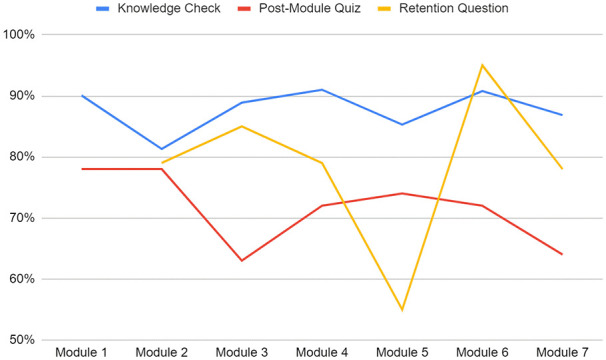
Results: 41 clinicians participated in the program. 100% reported high satisfaction and intention to apply learnings in practice. CVD knowledge and confidence increased among participants immediately post-course, with sustained improvements at a 6-month follow-up. QI teams achieved measurable improvements in clinical metrics and evidence-based CVD care practices through Plan-Do-Study-Act (PDSA) cycles, including an increase in optimized statin therapy rates from 72% to 86%. The clinical course also increased statin prescribing, with participating providers prescribing significantly more statins in the 6 months following the course than the 6 months before. Patients of participating clinicians experienced improved health outcomes, as evidenced by reductions in systolic blood pressure.
Conclusion: These findings illustrate the potential of academic medical centers collaborating with rural primary care clinics to address health disparities through the ECHO+ model, which combines tele-education and QI to enhance clinician capacity and improve population health outcomes.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


