Nikolay Belev, Andres Tein, Giuseppe Mangialardi, Alessandra Nuti, Giovanni Marino Merlo, Simona Scartoni, Monica Bertolotti, Margherita Lerro, Stefano Margaritora
{"title":"一项随机、观察者盲、主动对照的IIIb期研究,比较IV/口服德拉沙星固定剂量单药治疗与最佳治疗在微生物富集人群中手术部位感染:DRESS研究。","authors":"Nikolay Belev, Andres Tein, Giuseppe Mangialardi, Alessandra Nuti, Giovanni Marino Merlo, Simona Scartoni, Monica Bertolotti, Margherita Lerro, Stefano Margaritora","doi":"10.1093/ofid/ofaf476","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical site infections (SSIs) are the most common skin and skin structure infections and are mostly polymicrobial, requiring hospitalization and broad-spectrum antibiotics. This clinical trial evaluated the noninferiority of delafloxacin vs best available therapy (BAT) for the treatment of superficial or deep incisional SSI following a cardiothoracic/related leg or abdominal surgical procedure.</p><p><strong>Methods: </strong>In this randomized, observer-blinded, active-controlled, parallel-group, multicenter, phase IIIb study, patients with SSI were randomized 1:1 to receive delafloxacin 300 mg intravenous (IV)/450 mg oral (OS) or BAT IV/OS (vancomycin or linezolid for cardiothoracic SSI, piperacillin/tazobactam or tigecycline for abdominal SSI). The primary end point was clinical success, defined as the clinical response (cure or improved) at test of cure (TOC), performed 7-14 days after end of treatment (EOT) visit. Secondary end points were clinical success at EOT, sustained clinical response at last follow-up (LFU), microbiological response, and safety.</p><p><strong>Results: </strong>Thi study enrolled 266 patients (delafloxacin = 134; BAT = 132) with comparable baseline characteristics between the 2 treatment arms. Delafloxacin clinical success was noninferior vs BAT at TOC visit (91.8% vs 90.2%, respectively). Similar efficacy was confirmed at LFU (91.8% delafloxacin; 87.9% BAT). Comparable microbiological response was obtained with delafloxacin (89.5%) and BAT (79.4%). Delafloxacin and BAT demonstrated comparable treatment adverse event rates (23.9% and 19.7%, respectively), mostly mild-to-moderate gastrointestinal reactions.</p><p><strong>Conclusions: </strong>This study provided new data on delafloxacin in SSIs, covering the need for effective empiric treatment against the wide spectrum of pathogens involved in these infections.</p><p><strong>Clinical trials registration: </strong>NCT04042077; 2018-001082-17 (EudraCT).</p>","PeriodicalId":19517,"journal":{"name":"Open Forum Infectious Diseases","volume":"12 9","pages":"ofaf476"},"PeriodicalIF":3.8000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406695/pdf/","citationCount":"0","resultStr":"{\"title\":\"A Randomized, Observer-Blinded, Active-Controlled, Phase IIIb Study to Compare IV/Oral Delafloxacin Fixed-Dose Monotherapy With Best Available Treatments in a Microbiologically Enriched Population With Surgical Site Infections: The DRESS Study.\",\"authors\":\"Nikolay Belev, Andres Tein, Giuseppe Mangialardi, Alessandra Nuti, Giovanni Marino Merlo, Simona Scartoni, Monica Bertolotti, Margherita Lerro, Stefano Margaritora\",\"doi\":\"10.1093/ofid/ofaf476\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Surgical site infections (SSIs) are the most common skin and skin structure infections and are mostly polymicrobial, requiring hospitalization and broad-spectrum antibiotics. This clinical trial evaluated the noninferiority of delafloxacin vs best available therapy (BAT) for the treatment of superficial or deep incisional SSI following a cardiothoracic/related leg or abdominal surgical procedure.</p><p><strong>Methods: </strong>In this randomized, observer-blinded, active-controlled, parallel-group, multicenter, phase IIIb study, patients with SSI were randomized 1:1 to receive delafloxacin 300 mg intravenous (IV)/450 mg oral (OS) or BAT IV/OS (vancomycin or linezolid for cardiothoracic SSI, piperacillin/tazobactam or tigecycline for abdominal SSI). The primary end point was clinical success, defined as the clinical response (cure or improved) at test of cure (TOC), performed 7-14 days after end of treatment (EOT) visit. Secondary end points were clinical success at EOT, sustained clinical response at last follow-up (LFU), microbiological response, and safety.</p><p><strong>Results: </strong>Thi study enrolled 266 patients (delafloxacin = 134; BAT = 132) with comparable baseline characteristics between the 2 treatment arms. Delafloxacin clinical success was noninferior vs BAT at TOC visit (91.8% vs 90.2%, respectively). Similar efficacy was confirmed at LFU (91.8% delafloxacin; 87.9% BAT). Comparable microbiological response was obtained with delafloxacin (89.5%) and BAT (79.4%). Delafloxacin and BAT demonstrated comparable treatment adverse event rates (23.9% and 19.7%, respectively), mostly mild-to-moderate gastrointestinal reactions.</p><p><strong>Conclusions: </strong>This study provided new data on delafloxacin in SSIs, covering the need for effective empiric treatment against the wide spectrum of pathogens involved in these infections.</p><p><strong>Clinical trials registration: </strong>NCT04042077; 2018-001082-17 (EudraCT).</p>\",\"PeriodicalId\":19517,\"journal\":{\"name\":\"Open Forum Infectious Diseases\",\"volume\":\"12 9\",\"pages\":\"ofaf476\"},\"PeriodicalIF\":3.8000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406695/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Open Forum Infectious Diseases\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ofid/ofaf476\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"IMMUNOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Open Forum Infectious Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ofid/ofaf476","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:手术部位感染(ssi)是最常见的皮肤和皮肤结构感染,多为多微生物感染,需要住院治疗和使用广谱抗生素。该临床试验评估了德拉沙星与最佳可用疗法(BAT)在治疗胸外科/相关腿部或腹部手术后浅表或深切口SSI的非劣效性。方法:在这项随机、观察盲、主动对照、平行组、多中心、IIIb期研究中,SSI患者按1:1的比例随机接受德拉沙星300 mg静脉注射(IV)/450 mg口服(OS)或BAT IV/OS(万古霉素或利奈唑胺用于胸外科SSI,哌拉西林/他唑巴坦或替加环素用于腹部SSI)。主要终点是临床成功,定义为在治疗结束(EOT)访问后7-14天进行的治愈测试(TOC)的临床反应(治愈或改善)。次要终点是EOT的临床成功,最后随访时的持续临床反应(LFU),微生物反应和安全性。结果:本研究纳入266例患者(delafloxacin = 134; BAT = 132),两个治疗组的基线特征可比较。在TOC就诊时,与BAT相比,德拉沙星的临床成功率不差(分别为91.8%和90.2%)。LFU的疗效相似(delafloxacin 91.8%; BAT 87.9%)。delafloxacin(89.5%)和BAT(79.4%)的微生物反应相当。德拉沙星和BAT表现出相当的治疗不良事件发生率(分别为23.9%和19.7%),主要是轻至中度胃肠道反应。结论:本研究提供了delafloxacin在ssi中的新数据,涵盖了针对这些感染涉及的广泛病原体的有效经验性治疗的需求。临床试验注册:NCT04042077;2018-001082-17 (EudraCT)。
A Randomized, Observer-Blinded, Active-Controlled, Phase IIIb Study to Compare IV/Oral Delafloxacin Fixed-Dose Monotherapy With Best Available Treatments in a Microbiologically Enriched Population With Surgical Site Infections: The DRESS Study.
Background: Surgical site infections (SSIs) are the most common skin and skin structure infections and are mostly polymicrobial, requiring hospitalization and broad-spectrum antibiotics. This clinical trial evaluated the noninferiority of delafloxacin vs best available therapy (BAT) for the treatment of superficial or deep incisional SSI following a cardiothoracic/related leg or abdominal surgical procedure.
Methods: In this randomized, observer-blinded, active-controlled, parallel-group, multicenter, phase IIIb study, patients with SSI were randomized 1:1 to receive delafloxacin 300 mg intravenous (IV)/450 mg oral (OS) or BAT IV/OS (vancomycin or linezolid for cardiothoracic SSI, piperacillin/tazobactam or tigecycline for abdominal SSI). The primary end point was clinical success, defined as the clinical response (cure or improved) at test of cure (TOC), performed 7-14 days after end of treatment (EOT) visit. Secondary end points were clinical success at EOT, sustained clinical response at last follow-up (LFU), microbiological response, and safety.
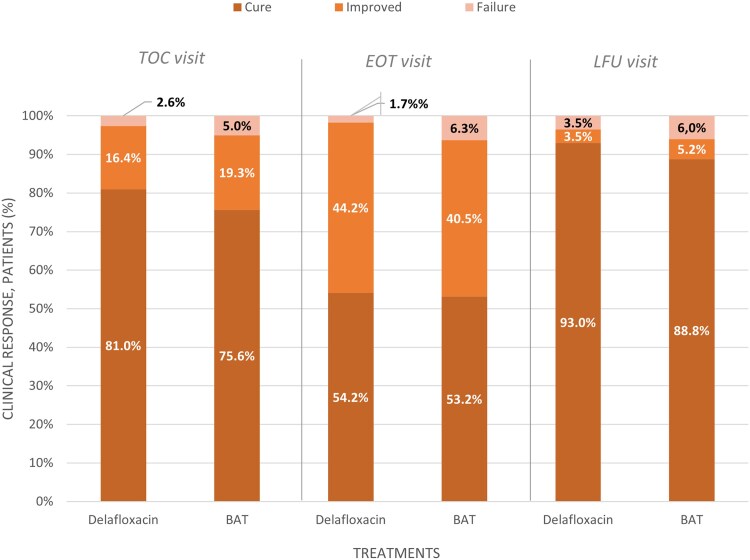
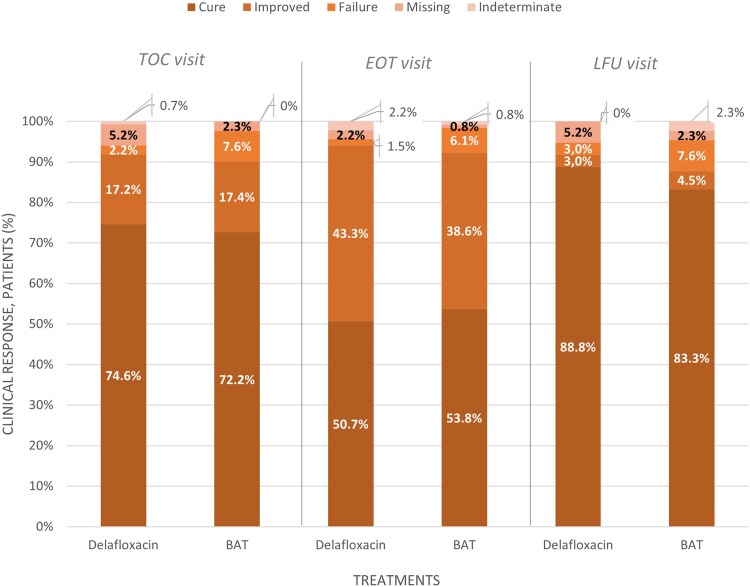
Results: Thi study enrolled 266 patients (delafloxacin = 134; BAT = 132) with comparable baseline characteristics between the 2 treatment arms. Delafloxacin clinical success was noninferior vs BAT at TOC visit (91.8% vs 90.2%, respectively). Similar efficacy was confirmed at LFU (91.8% delafloxacin; 87.9% BAT). Comparable microbiological response was obtained with delafloxacin (89.5%) and BAT (79.4%). Delafloxacin and BAT demonstrated comparable treatment adverse event rates (23.9% and 19.7%, respectively), mostly mild-to-moderate gastrointestinal reactions.
Conclusions: This study provided new data on delafloxacin in SSIs, covering the need for effective empiric treatment against the wide spectrum of pathogens involved in these infections.
期刊介绍:
Open Forum Infectious Diseases provides a global forum for the publication of clinical, translational, and basic research findings in a fully open access, online journal environment. The journal reflects the broad diversity of the field of infectious diseases, and focuses on the intersection of biomedical science and clinical practice, with a particular emphasis on knowledge that holds the potential to improve patient care in populations around the world. Fully peer-reviewed, OFID supports the international community of infectious diseases experts by providing a venue for articles that further the understanding of all aspects of infectious diseases.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


