{"title":"红曲米致严重横纹肌溶解合并急性肾损伤及呼吸衰竭1例。","authors":"Pengmin Zhou, Yucai Hong, Huabo Cai, Xiaoyu Zhou, Shunpeng He, Haotian Zhou, Jie Yang, Pengpeng Chen, Boming Xia, Xiong Lei, Suibi Yang, Zhongheng Zhang","doi":"10.3389/fmed.2025.1634047","DOIUrl":null,"url":null,"abstract":"<p><p>Red yeast rice (RYR), a commonly used supplement with statin-like properties, is generally considered safe but may cause severe adverse effects such as rhabdomyolysis. We report a rare case of severe RYR-induced rhabdomyolysis complicated by acute kidney injury (AKI) and respiratory failure, with diaphragmatic dysfunction as a key contributing factor. A 78-year-old woman developed progressive proximal muscle weakness, dyspnea, and tea-colored urine after taking RYR (2 g/day) for 1 month. She rapidly progressed to respiratory failure requiring intubation and mechanical ventilation. Laboratory tests showed a peak creatine kinase (CK) of 112,985 U/L, serum myoglobin (>3,000 μg/L), and AKI. Bedside ultrasound demonstrated diaphragmatic dysfunction, while electromyography (EMG) revealed preserved nerve conduction. Myositis-specific and paraneoplastic antibody panels were negative. She received continuous renal replacement therapy (CRRT), plasma exchange (PE), hemoperfusion (HP), and supportive care. During hospitalization, she developed deep vein thrombosis (DVT), pneumonia, and ileus, all of which resolved with treatment. At discharge, she had been weaned from mechanical ventilation and had partially recovered renal and muscle function. At follow-up, she was stable, ambulating, and performing daily functions without symptom recurrence. Although her initial presentation mimicked immune-mediated necrotizing myopathy (IMNM), the absence of myositis-specific antibodies and clinical improvement without immunosuppressive therapy supported a diagnosis of toxic rhabdomyolysis. This case highlights the importance of recognizing supplement-related toxicity and initiating timely organ-targeted supportive care. This appears to be the first reported case of RYR-induced rhabdomyolysis complicated by both AKI and respiratory failure from diaphragmatic dysfunction.</p>","PeriodicalId":12488,"journal":{"name":"Frontiers in Medicine","volume":"12 ","pages":"1634047"},"PeriodicalIF":3.1000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404951/pdf/","citationCount":"0","resultStr":"{\"title\":\"Red yeast rice-induced severe rhabdomyolysis complicated by acute kidney injury and respiratory failure: a case report.\",\"authors\":\"Pengmin Zhou, Yucai Hong, Huabo Cai, Xiaoyu Zhou, Shunpeng He, Haotian Zhou, Jie Yang, Pengpeng Chen, Boming Xia, Xiong Lei, Suibi Yang, Zhongheng Zhang\",\"doi\":\"10.3389/fmed.2025.1634047\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Red yeast rice (RYR), a commonly used supplement with statin-like properties, is generally considered safe but may cause severe adverse effects such as rhabdomyolysis. We report a rare case of severe RYR-induced rhabdomyolysis complicated by acute kidney injury (AKI) and respiratory failure, with diaphragmatic dysfunction as a key contributing factor. A 78-year-old woman developed progressive proximal muscle weakness, dyspnea, and tea-colored urine after taking RYR (2 g/day) for 1 month. She rapidly progressed to respiratory failure requiring intubation and mechanical ventilation. Laboratory tests showed a peak creatine kinase (CK) of 112,985 U/L, serum myoglobin (>3,000 μg/L), and AKI. Bedside ultrasound demonstrated diaphragmatic dysfunction, while electromyography (EMG) revealed preserved nerve conduction. Myositis-specific and paraneoplastic antibody panels were negative. She received continuous renal replacement therapy (CRRT), plasma exchange (PE), hemoperfusion (HP), and supportive care. During hospitalization, she developed deep vein thrombosis (DVT), pneumonia, and ileus, all of which resolved with treatment. At discharge, she had been weaned from mechanical ventilation and had partially recovered renal and muscle function. At follow-up, she was stable, ambulating, and performing daily functions without symptom recurrence. Although her initial presentation mimicked immune-mediated necrotizing myopathy (IMNM), the absence of myositis-specific antibodies and clinical improvement without immunosuppressive therapy supported a diagnosis of toxic rhabdomyolysis. This case highlights the importance of recognizing supplement-related toxicity and initiating timely organ-targeted supportive care. This appears to be the first reported case of RYR-induced rhabdomyolysis complicated by both AKI and respiratory failure from diaphragmatic dysfunction.</p>\",\"PeriodicalId\":12488,\"journal\":{\"name\":\"Frontiers in Medicine\",\"volume\":\"12 \",\"pages\":\"1634047\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2025-08-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404951/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3389/fmed.2025.1634047\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/fmed.2025.1634047","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Red yeast rice-induced severe rhabdomyolysis complicated by acute kidney injury and respiratory failure: a case report.
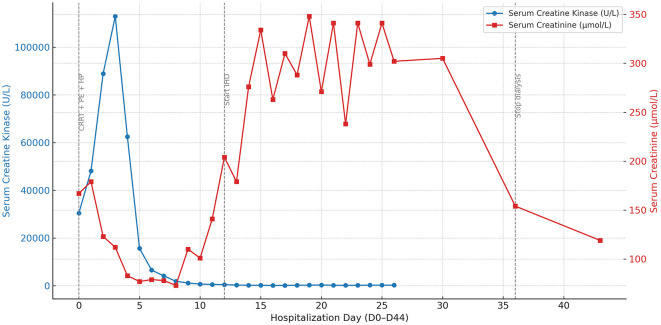
Red yeast rice (RYR), a commonly used supplement with statin-like properties, is generally considered safe but may cause severe adverse effects such as rhabdomyolysis. We report a rare case of severe RYR-induced rhabdomyolysis complicated by acute kidney injury (AKI) and respiratory failure, with diaphragmatic dysfunction as a key contributing factor. A 78-year-old woman developed progressive proximal muscle weakness, dyspnea, and tea-colored urine after taking RYR (2 g/day) for 1 month. She rapidly progressed to respiratory failure requiring intubation and mechanical ventilation. Laboratory tests showed a peak creatine kinase (CK) of 112,985 U/L, serum myoglobin (>3,000 μg/L), and AKI. Bedside ultrasound demonstrated diaphragmatic dysfunction, while electromyography (EMG) revealed preserved nerve conduction. Myositis-specific and paraneoplastic antibody panels were negative. She received continuous renal replacement therapy (CRRT), plasma exchange (PE), hemoperfusion (HP), and supportive care. During hospitalization, she developed deep vein thrombosis (DVT), pneumonia, and ileus, all of which resolved with treatment. At discharge, she had been weaned from mechanical ventilation and had partially recovered renal and muscle function. At follow-up, she was stable, ambulating, and performing daily functions without symptom recurrence. Although her initial presentation mimicked immune-mediated necrotizing myopathy (IMNM), the absence of myositis-specific antibodies and clinical improvement without immunosuppressive therapy supported a diagnosis of toxic rhabdomyolysis. This case highlights the importance of recognizing supplement-related toxicity and initiating timely organ-targeted supportive care. This appears to be the first reported case of RYR-induced rhabdomyolysis complicated by both AKI and respiratory failure from diaphragmatic dysfunction.
期刊介绍:
Frontiers in Medicine publishes rigorously peer-reviewed research linking basic research to clinical practice and patient care, as well as translating scientific advances into new therapies and diagnostic tools. Led by an outstanding Editorial Board of international experts, this multidisciplinary open-access journal is at the forefront of disseminating and communicating scientific knowledge and impactful discoveries to researchers, academics, clinicians and the public worldwide.
In addition to papers that provide a link between basic research and clinical practice, a particular emphasis is given to studies that are directly relevant to patient care. In this spirit, the journal publishes the latest research results and medical knowledge that facilitate the translation of scientific advances into new therapies or diagnostic tools. The full listing of the Specialty Sections represented by Frontiers in Medicine is as listed below. As well as the established medical disciplines, Frontiers in Medicine is launching new sections that together will facilitate
- the use of patient-reported outcomes under real world conditions
- the exploitation of big data and the use of novel information and communication tools in the assessment of new medicines
- the scientific bases for guidelines and decisions from regulatory authorities
- access to medicinal products and medical devices worldwide
- addressing the grand health challenges around the world

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


