Timothy Ryan, Laura Luttrell, Amit Shah, Kaitlyn Lam, Peter Dias, Aws Jasim, Andrew Laycock, Vimal Patel
{"title":"长期使用羟氯喹导致心肌病和传导异常1例报告。","authors":"Timothy Ryan, Laura Luttrell, Amit Shah, Kaitlyn Lam, Peter Dias, Aws Jasim, Andrew Laycock, Vimal Patel","doi":"10.1093/ehjcr/ytaf377","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Diagnosing the cause of undifferentiated left ventricular hypertrophy (LVH) in a patient with progressive heart failure symptoms can present a diagnostic challenge, with potential for both inherited and acquired aetiologies. Hydroxychloroquine-induced cardiomyopathy (HCQ-CM) is a rare complication of long-term hydroxychloroquine use. This case report highlights its clinical presentation, key differential diagnoses, and treatment strategies.</p><p><strong>Case summary: </strong>A 56-year-old female with a longstanding history of systemic lupus erythematosus presented with progressive dyspnoea, fatigue, and fluid overload. Initial investigation revealed LVH with restrictive physiology, elevated cardiac biomarkers, and non-specific findings on echocardiography suggestive of an infiltrative cardiomyopathy. The diagnosis remained uncertain until an endomyocardial biopsy (EMB) confirmed HCQ-CM, characterized by the presence of curvilinear inclusion bodies. Following cessation of HCQ, there was a significant clinical improvement, with the patient achieving NYHA class I status at 6 months follow-up.</p><p><strong>Conclusion: </strong>This case highlights the critical importance of considering HCQ-CM, in the differential diagnosis of unexplained heart failure and LVH in patients on long-term HCQ therapy. A multi-parametric diagnostic approach-including EMB and genetic testing where appropriate-is essential to identify potentially reversible causes of cardiomyopathy and enable timely therapeutic adjustments.</p>","PeriodicalId":11910,"journal":{"name":"European Heart Journal: Case Reports","volume":"9 9","pages":"ytaf377"},"PeriodicalIF":0.8000,"publicationDate":"2025-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12405751/pdf/","citationCount":"0","resultStr":"{\"title\":\"Long-term hydroxychloroquine use resulting in cardiomyopathy and conduction abnormalities: a case report.\",\"authors\":\"Timothy Ryan, Laura Luttrell, Amit Shah, Kaitlyn Lam, Peter Dias, Aws Jasim, Andrew Laycock, Vimal Patel\",\"doi\":\"10.1093/ehjcr/ytaf377\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Diagnosing the cause of undifferentiated left ventricular hypertrophy (LVH) in a patient with progressive heart failure symptoms can present a diagnostic challenge, with potential for both inherited and acquired aetiologies. Hydroxychloroquine-induced cardiomyopathy (HCQ-CM) is a rare complication of long-term hydroxychloroquine use. This case report highlights its clinical presentation, key differential diagnoses, and treatment strategies.</p><p><strong>Case summary: </strong>A 56-year-old female with a longstanding history of systemic lupus erythematosus presented with progressive dyspnoea, fatigue, and fluid overload. Initial investigation revealed LVH with restrictive physiology, elevated cardiac biomarkers, and non-specific findings on echocardiography suggestive of an infiltrative cardiomyopathy. The diagnosis remained uncertain until an endomyocardial biopsy (EMB) confirmed HCQ-CM, characterized by the presence of curvilinear inclusion bodies. Following cessation of HCQ, there was a significant clinical improvement, with the patient achieving NYHA class I status at 6 months follow-up.</p><p><strong>Conclusion: </strong>This case highlights the critical importance of considering HCQ-CM, in the differential diagnosis of unexplained heart failure and LVH in patients on long-term HCQ therapy. A multi-parametric diagnostic approach-including EMB and genetic testing where appropriate-is essential to identify potentially reversible causes of cardiomyopathy and enable timely therapeutic adjustments.</p>\",\"PeriodicalId\":11910,\"journal\":{\"name\":\"European Heart Journal: Case Reports\",\"volume\":\"9 9\",\"pages\":\"ytaf377\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2025-09-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12405751/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal: Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjcr/ytaf377\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/9/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal: Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjcr/ytaf377","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/9/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Long-term hydroxychloroquine use resulting in cardiomyopathy and conduction abnormalities: a case report.
Background: Diagnosing the cause of undifferentiated left ventricular hypertrophy (LVH) in a patient with progressive heart failure symptoms can present a diagnostic challenge, with potential for both inherited and acquired aetiologies. Hydroxychloroquine-induced cardiomyopathy (HCQ-CM) is a rare complication of long-term hydroxychloroquine use. This case report highlights its clinical presentation, key differential diagnoses, and treatment strategies.
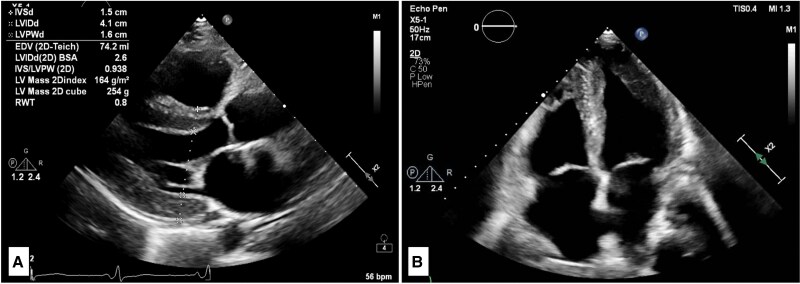
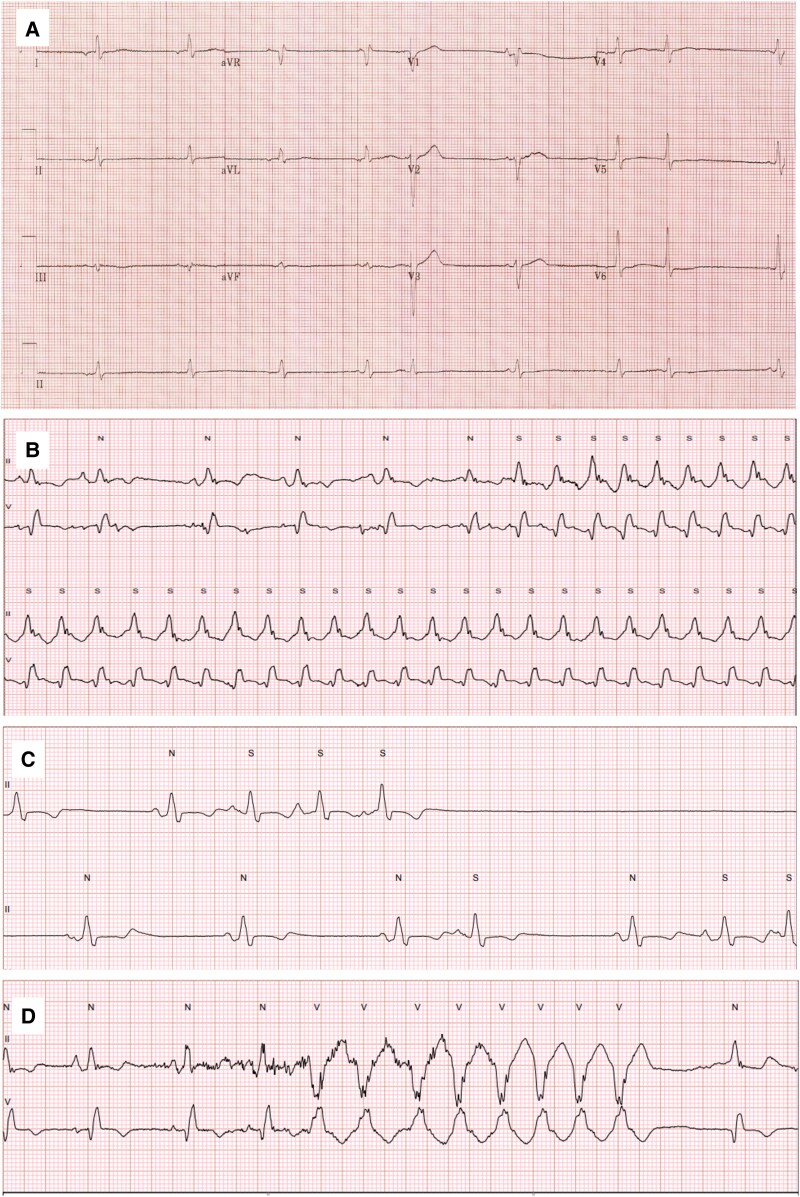
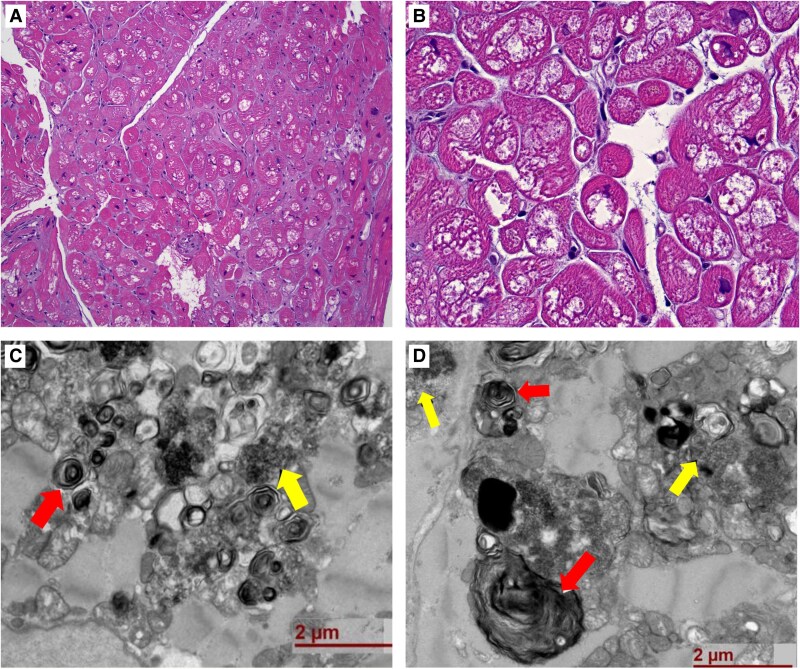
Case summary: A 56-year-old female with a longstanding history of systemic lupus erythematosus presented with progressive dyspnoea, fatigue, and fluid overload. Initial investigation revealed LVH with restrictive physiology, elevated cardiac biomarkers, and non-specific findings on echocardiography suggestive of an infiltrative cardiomyopathy. The diagnosis remained uncertain until an endomyocardial biopsy (EMB) confirmed HCQ-CM, characterized by the presence of curvilinear inclusion bodies. Following cessation of HCQ, there was a significant clinical improvement, with the patient achieving NYHA class I status at 6 months follow-up.
Conclusion: This case highlights the critical importance of considering HCQ-CM, in the differential diagnosis of unexplained heart failure and LVH in patients on long-term HCQ therapy. A multi-parametric diagnostic approach-including EMB and genetic testing where appropriate-is essential to identify potentially reversible causes of cardiomyopathy and enable timely therapeutic adjustments.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


