{"title":"腹腔镜经囊胆总管探查的预后及相关危险因素。","authors":"Deng-Sheng Zhu, Zhen Zhang, Xiao-Rui Huang, Jing-Zhao Zhang, Zhi-Wei Zhang, Xin-Yi Guo, Huan Zheng, Tong Guo, Ya-Hong Yu","doi":"10.3748/wjg.v31.i31.109994","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Textbook outcome (TO), an emerging composite metric for surgical quality assessment, has recently gained recognition for evaluating perioperative results. Laparoscopic transcystic common bile duct exploration (LTCBDE) has become a widely adopted minimally invasive technique for treating cholecystolithiasis with choledocholithiasis. Despite its growing clinical application, TO has not yet been formally defined for LTCBDE, nor have its failure-associated risk factors been systematically examined.</p><p><strong>Aim: </strong>To define TO for LTCBDE, establish standardized criteria, and identify risk factors for TO failure <i>via</i> logistic regression.</p><p><strong>Methods: </strong>A retrospective cohort of 388 patients who underwent LTCBDE in combination with laparoscopic cholecystectomy at the Department of Biliopancreatic Surgery, Tongji Hospital, from January 2018 to October 2024, was analyzed. The study delineated TO criteria for LTCBDE, calculated the rate of TO achievement, and employed logistic regression to determine independent predictors of TO failure.</p><p><strong>Results: </strong>TO was defined as the absence of the following seven criteria: Conversion to open surgery, postoperative complications (Clavien-Dindo grade ≥ 2), biliary leakage (International Study Group of Pancreatic Surgery/International Study Group of Liver Surgery grade B/C), delayed removal of drainage tube (> 4 days), postoperative interventions, prolonged length of stay (> 7 days), and 30-day readmission or mortality. Among 388 patients, 276 (71.1%) achieved TO. The primary causes of TO failure included delayed removal of drainage tube (94 cases, 83.9%), prolonged length of stay (50 cases, 44.6%). Multivariate analysis revealed four independent risk factors for TO failure: Preoperative endoscopic retrograde cholangiopancreatography (<i>P</i> = 0.022), advanced age (<i>P</i> = 0.010), prolonged anesthesia time (<i>P</i> < 0.001), and elevated preoperative alkaline phosphatase levels (<i>P</i> = 0.048).</p><p><strong>Conclusion: </strong>These findings suggest that applying the concept of TO to LTCBDE enhances surgical quality evaluation and supports early identification of high-risk patients, facilitating personalized clinical decisions and optimizing individual management.</p>","PeriodicalId":23778,"journal":{"name":"World Journal of Gastroenterology","volume":"31 31","pages":"109994"},"PeriodicalIF":5.4000,"publicationDate":"2025-08-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400204/pdf/","citationCount":"0","resultStr":"{\"title\":\"Textbook outcome and associated risk factors in laparoscopic transcystic common bile duct exploration.\",\"authors\":\"Deng-Sheng Zhu, Zhen Zhang, Xiao-Rui Huang, Jing-Zhao Zhang, Zhi-Wei Zhang, Xin-Yi Guo, Huan Zheng, Tong Guo, Ya-Hong Yu\",\"doi\":\"10.3748/wjg.v31.i31.109994\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Textbook outcome (TO), an emerging composite metric for surgical quality assessment, has recently gained recognition for evaluating perioperative results. Laparoscopic transcystic common bile duct exploration (LTCBDE) has become a widely adopted minimally invasive technique for treating cholecystolithiasis with choledocholithiasis. Despite its growing clinical application, TO has not yet been formally defined for LTCBDE, nor have its failure-associated risk factors been systematically examined.</p><p><strong>Aim: </strong>To define TO for LTCBDE, establish standardized criteria, and identify risk factors for TO failure <i>via</i> logistic regression.</p><p><strong>Methods: </strong>A retrospective cohort of 388 patients who underwent LTCBDE in combination with laparoscopic cholecystectomy at the Department of Biliopancreatic Surgery, Tongji Hospital, from January 2018 to October 2024, was analyzed. The study delineated TO criteria for LTCBDE, calculated the rate of TO achievement, and employed logistic regression to determine independent predictors of TO failure.</p><p><strong>Results: </strong>TO was defined as the absence of the following seven criteria: Conversion to open surgery, postoperative complications (Clavien-Dindo grade ≥ 2), biliary leakage (International Study Group of Pancreatic Surgery/International Study Group of Liver Surgery grade B/C), delayed removal of drainage tube (> 4 days), postoperative interventions, prolonged length of stay (> 7 days), and 30-day readmission or mortality. Among 388 patients, 276 (71.1%) achieved TO. The primary causes of TO failure included delayed removal of drainage tube (94 cases, 83.9%), prolonged length of stay (50 cases, 44.6%). Multivariate analysis revealed four independent risk factors for TO failure: Preoperative endoscopic retrograde cholangiopancreatography (<i>P</i> = 0.022), advanced age (<i>P</i> = 0.010), prolonged anesthesia time (<i>P</i> < 0.001), and elevated preoperative alkaline phosphatase levels (<i>P</i> = 0.048).</p><p><strong>Conclusion: </strong>These findings suggest that applying the concept of TO to LTCBDE enhances surgical quality evaluation and supports early identification of high-risk patients, facilitating personalized clinical decisions and optimizing individual management.</p>\",\"PeriodicalId\":23778,\"journal\":{\"name\":\"World Journal of Gastroenterology\",\"volume\":\"31 31\",\"pages\":\"109994\"},\"PeriodicalIF\":5.4000,\"publicationDate\":\"2025-08-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400204/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.3748/wjg.v31.i31.109994\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3748/wjg.v31.i31.109994","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Textbook outcome and associated risk factors in laparoscopic transcystic common bile duct exploration.
Background: Textbook outcome (TO), an emerging composite metric for surgical quality assessment, has recently gained recognition for evaluating perioperative results. Laparoscopic transcystic common bile duct exploration (LTCBDE) has become a widely adopted minimally invasive technique for treating cholecystolithiasis with choledocholithiasis. Despite its growing clinical application, TO has not yet been formally defined for LTCBDE, nor have its failure-associated risk factors been systematically examined.
Aim: To define TO for LTCBDE, establish standardized criteria, and identify risk factors for TO failure via logistic regression.
Methods: A retrospective cohort of 388 patients who underwent LTCBDE in combination with laparoscopic cholecystectomy at the Department of Biliopancreatic Surgery, Tongji Hospital, from January 2018 to October 2024, was analyzed. The study delineated TO criteria for LTCBDE, calculated the rate of TO achievement, and employed logistic regression to determine independent predictors of TO failure.
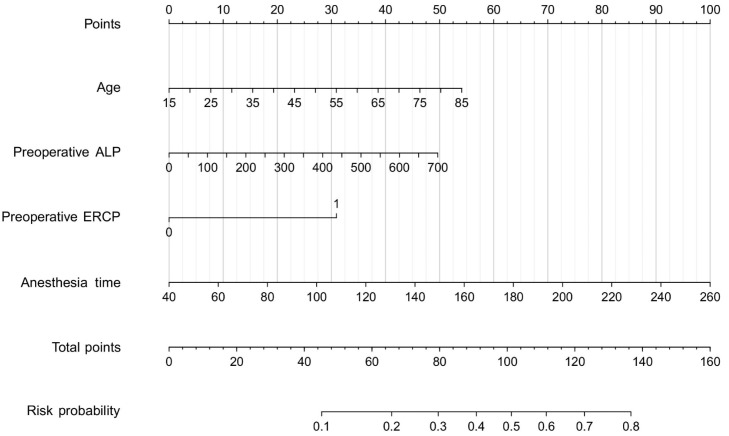
Results: TO was defined as the absence of the following seven criteria: Conversion to open surgery, postoperative complications (Clavien-Dindo grade ≥ 2), biliary leakage (International Study Group of Pancreatic Surgery/International Study Group of Liver Surgery grade B/C), delayed removal of drainage tube (> 4 days), postoperative interventions, prolonged length of stay (> 7 days), and 30-day readmission or mortality. Among 388 patients, 276 (71.1%) achieved TO. The primary causes of TO failure included delayed removal of drainage tube (94 cases, 83.9%), prolonged length of stay (50 cases, 44.6%). Multivariate analysis revealed four independent risk factors for TO failure: Preoperative endoscopic retrograde cholangiopancreatography (P = 0.022), advanced age (P = 0.010), prolonged anesthesia time (P < 0.001), and elevated preoperative alkaline phosphatase levels (P = 0.048).
Conclusion: These findings suggest that applying the concept of TO to LTCBDE enhances surgical quality evaluation and supports early identification of high-risk patients, facilitating personalized clinical decisions and optimizing individual management.
期刊介绍:
The primary aims of the WJG are to improve diagnostic, therapeutic and preventive modalities and the skills of clinicians and to guide clinical practice in gastroenterology and hepatology.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


