{"title":"小腿大量淋巴水肿并发严重皮肤硬化症。","authors":"Kotaro Suehiro, Hiroyuki Takasu, Seiko Fujino, Takasuke Harada, Makoto Samura, Yuriko Takeuchi, Takahiro Mizoguchi, Hiroshi Kurazumi, Ryo Suzuki, Kimikazu Hamano","doi":"10.70352/scrj.cr.25-0375","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Lymphedema is generally managed with conservative therapy. However, in cases of severe fibrosclerotic lymphedema, debulking surgery is required, although rarely. We present a case of massive lymphedema in the left calf complicated by severe skin fibrosclerosis that was successfully managed with debulking surgery.</p><p><strong>Case presentation: </strong>A 58-year-old woman presented to our clinic with bilateral leg swelling, which was particularly massive in the left calf. She could hardly walk independently and experienced cellulitis 2 to 4 times a year. The patient was admitted, and aggressive decongestion with compression therapy was attempted initially. However, this was unsuccessful due to severe skin hardening caused by abnormal dermal thickening. We then performed partial subcutaneous tissue resection and wrapping with the redundant skin, but this resulted in extensive skin necrosis. Finally, resection of the whole skin and subcutaneous tissue down to the deep fascia in the left calf was performed, followed by split-thickness skin grafting harvested from the left thigh. At present, one year after the surgery, the patient is capable of performing light exercise and has not experienced a recurrence of cellulitis.</p><p><strong>Conclusions: </strong>When preoperative conservative therapy is unsuccessful due to severe skin fibrosclerosis, earlier surgical intervention, including debulking, is beneficial in the management of massive lymphedema.</p>","PeriodicalId":22096,"journal":{"name":"Surgical Case Reports","volume":"11 1","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404784/pdf/","citationCount":"0","resultStr":"{\"title\":\"Massive Lymphedema in the Calf Complicated by Severe Skin Fibrosclerosis.\",\"authors\":\"Kotaro Suehiro, Hiroyuki Takasu, Seiko Fujino, Takasuke Harada, Makoto Samura, Yuriko Takeuchi, Takahiro Mizoguchi, Hiroshi Kurazumi, Ryo Suzuki, Kimikazu Hamano\",\"doi\":\"10.70352/scrj.cr.25-0375\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Lymphedema is generally managed with conservative therapy. However, in cases of severe fibrosclerotic lymphedema, debulking surgery is required, although rarely. We present a case of massive lymphedema in the left calf complicated by severe skin fibrosclerosis that was successfully managed with debulking surgery.</p><p><strong>Case presentation: </strong>A 58-year-old woman presented to our clinic with bilateral leg swelling, which was particularly massive in the left calf. She could hardly walk independently and experienced cellulitis 2 to 4 times a year. The patient was admitted, and aggressive decongestion with compression therapy was attempted initially. However, this was unsuccessful due to severe skin hardening caused by abnormal dermal thickening. We then performed partial subcutaneous tissue resection and wrapping with the redundant skin, but this resulted in extensive skin necrosis. Finally, resection of the whole skin and subcutaneous tissue down to the deep fascia in the left calf was performed, followed by split-thickness skin grafting harvested from the left thigh. At present, one year after the surgery, the patient is capable of performing light exercise and has not experienced a recurrence of cellulitis.</p><p><strong>Conclusions: </strong>When preoperative conservative therapy is unsuccessful due to severe skin fibrosclerosis, earlier surgical intervention, including debulking, is beneficial in the management of massive lymphedema.</p>\",\"PeriodicalId\":22096,\"journal\":{\"name\":\"Surgical Case Reports\",\"volume\":\"11 1\",\"pages\":\"\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12404784/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Surgical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.70352/scrj.cr.25-0375\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/8/26 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.70352/scrj.cr.25-0375","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/8/26 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
Massive Lymphedema in the Calf Complicated by Severe Skin Fibrosclerosis.
Introduction: Lymphedema is generally managed with conservative therapy. However, in cases of severe fibrosclerotic lymphedema, debulking surgery is required, although rarely. We present a case of massive lymphedema in the left calf complicated by severe skin fibrosclerosis that was successfully managed with debulking surgery.
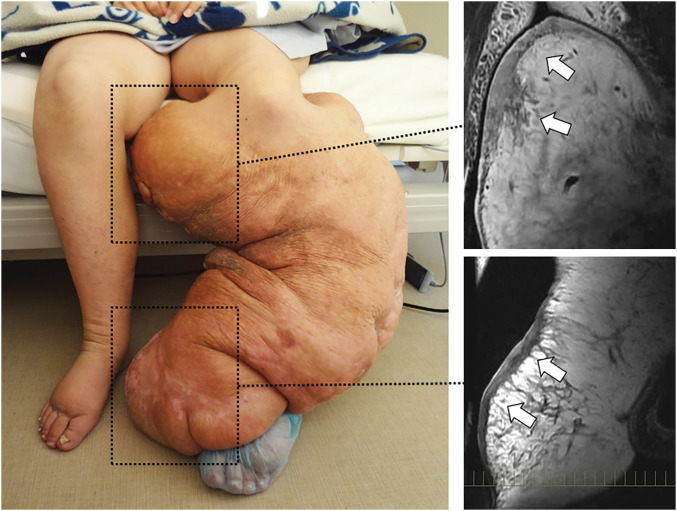
Case presentation: A 58-year-old woman presented to our clinic with bilateral leg swelling, which was particularly massive in the left calf. She could hardly walk independently and experienced cellulitis 2 to 4 times a year. The patient was admitted, and aggressive decongestion with compression therapy was attempted initially. However, this was unsuccessful due to severe skin hardening caused by abnormal dermal thickening. We then performed partial subcutaneous tissue resection and wrapping with the redundant skin, but this resulted in extensive skin necrosis. Finally, resection of the whole skin and subcutaneous tissue down to the deep fascia in the left calf was performed, followed by split-thickness skin grafting harvested from the left thigh. At present, one year after the surgery, the patient is capable of performing light exercise and has not experienced a recurrence of cellulitis.
Conclusions: When preoperative conservative therapy is unsuccessful due to severe skin fibrosclerosis, earlier surgical intervention, including debulking, is beneficial in the management of massive lymphedema.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


