{"title":"颅骨成形术中的地雷:先前未确诊的动脉瘤异常破裂。说明情况。","authors":"Aaron Miller, Julio Isidor, Liz Iglesias, Isaiah Miller, Aimee Weber, Ricardo Domingo, Alejandro Spiotta","doi":"10.3171/CASE25431","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Spontaneous rupture of an undiagnosed aneurysm during a neurosurgical procedure not aimed at treating it is exceedingly rare, although multiple intraoperative factors can contribute to this situation.</p><p><strong>Observations: </strong>A patient in his 20s with a history of a 60-cm3 left intraparenchymal hematoma treated via decompressive craniectomy in November 2024 presented in March 2025 with a first-time seizure. Keppra was initiated, and the patient was admitted for cranioplasty. During the procedure, the previously sunken brain suddenly developed severe edema, herniating through the craniectomy defect. Intraoperative ultrasound was negative for hematoma but showed a thick subarachnoid hemorrhage (SAH) in the sylvian fissure. Postoperative CT revealed diffuse SAH and hydrocephalus; an external ventricular drain was urgently placed. Angiography identified and aided in coiling of an ophthalmic aneurysm.</p><p><strong>Lessons: </strong>Several factors can precipitate intraoperative aneurysm rupture. Osmotic agents like mannitol can cause rapid intravascular fluid shifts, increasing hemodynamic stress across the aneurysm dome. Atmospheric pressure changes due to intraoperative manipulation can also alter extravascular forces on the aneurysm. Based on this experience, especially in young patients with prior unexplained hemorrhage, the authors advise careful use of mannitol and surgical technique. Surgeons should consider these risks in patients with known or suspected aneurysms to prevent catastrophic rupture. https://thejns.org/doi/10.3171/CASE25431.</p>","PeriodicalId":94098,"journal":{"name":"Journal of neurosurgery. Case lessons","volume":"10 9","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400849/pdf/","citationCount":"0","resultStr":"{\"title\":\"A landmine during cranioplasty: unusual rupture of a previously undiagnosed aneurysm. Illustrative case.\",\"authors\":\"Aaron Miller, Julio Isidor, Liz Iglesias, Isaiah Miller, Aimee Weber, Ricardo Domingo, Alejandro Spiotta\",\"doi\":\"10.3171/CASE25431\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Spontaneous rupture of an undiagnosed aneurysm during a neurosurgical procedure not aimed at treating it is exceedingly rare, although multiple intraoperative factors can contribute to this situation.</p><p><strong>Observations: </strong>A patient in his 20s with a history of a 60-cm3 left intraparenchymal hematoma treated via decompressive craniectomy in November 2024 presented in March 2025 with a first-time seizure. Keppra was initiated, and the patient was admitted for cranioplasty. During the procedure, the previously sunken brain suddenly developed severe edema, herniating through the craniectomy defect. Intraoperative ultrasound was negative for hematoma but showed a thick subarachnoid hemorrhage (SAH) in the sylvian fissure. Postoperative CT revealed diffuse SAH and hydrocephalus; an external ventricular drain was urgently placed. Angiography identified and aided in coiling of an ophthalmic aneurysm.</p><p><strong>Lessons: </strong>Several factors can precipitate intraoperative aneurysm rupture. Osmotic agents like mannitol can cause rapid intravascular fluid shifts, increasing hemodynamic stress across the aneurysm dome. Atmospheric pressure changes due to intraoperative manipulation can also alter extravascular forces on the aneurysm. Based on this experience, especially in young patients with prior unexplained hemorrhage, the authors advise careful use of mannitol and surgical technique. Surgeons should consider these risks in patients with known or suspected aneurysms to prevent catastrophic rupture. https://thejns.org/doi/10.3171/CASE25431.</p>\",\"PeriodicalId\":94098,\"journal\":{\"name\":\"Journal of neurosurgery. Case lessons\",\"volume\":\"10 9\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400849/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of neurosurgery. Case lessons\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3171/CASE25431\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of neurosurgery. Case lessons","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3171/CASE25431","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
A landmine during cranioplasty: unusual rupture of a previously undiagnosed aneurysm. Illustrative case.
Background: Spontaneous rupture of an undiagnosed aneurysm during a neurosurgical procedure not aimed at treating it is exceedingly rare, although multiple intraoperative factors can contribute to this situation.
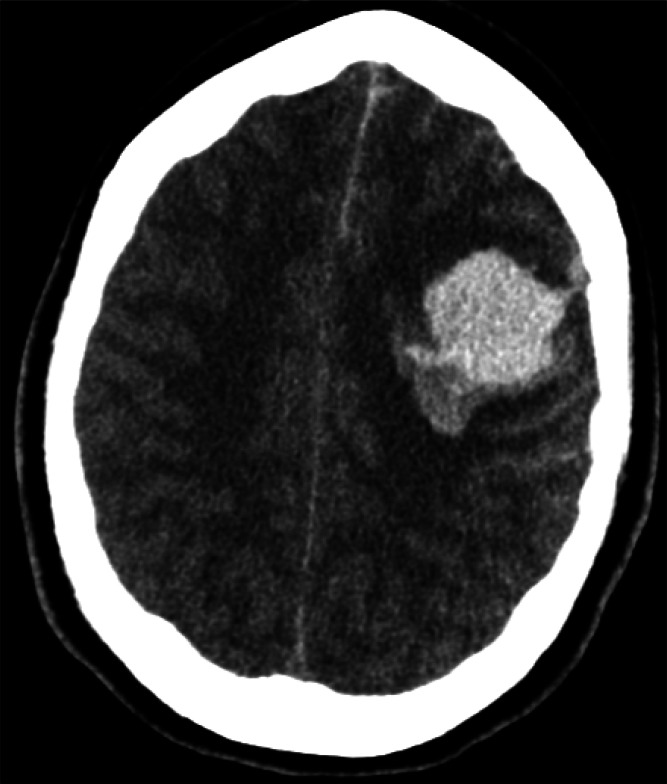
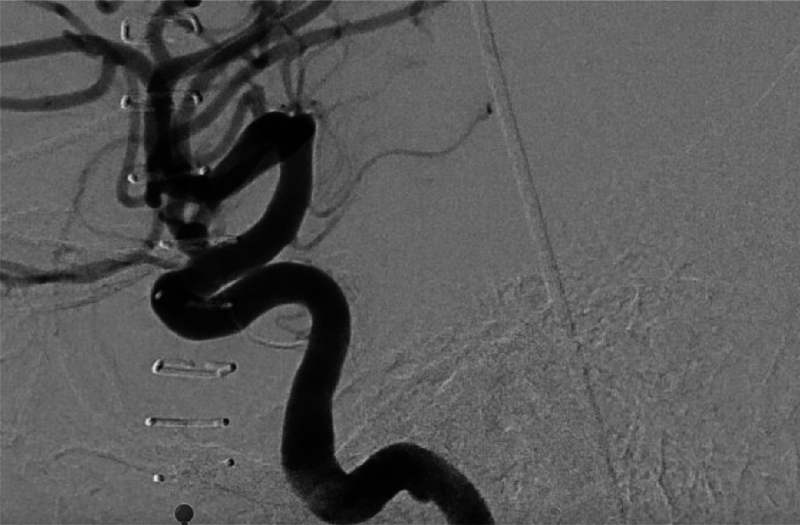
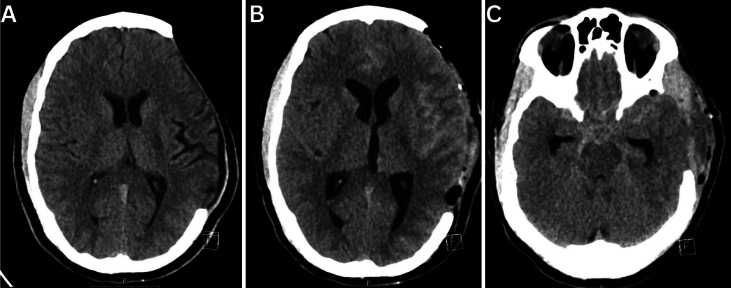
Observations: A patient in his 20s with a history of a 60-cm3 left intraparenchymal hematoma treated via decompressive craniectomy in November 2024 presented in March 2025 with a first-time seizure. Keppra was initiated, and the patient was admitted for cranioplasty. During the procedure, the previously sunken brain suddenly developed severe edema, herniating through the craniectomy defect. Intraoperative ultrasound was negative for hematoma but showed a thick subarachnoid hemorrhage (SAH) in the sylvian fissure. Postoperative CT revealed diffuse SAH and hydrocephalus; an external ventricular drain was urgently placed. Angiography identified and aided in coiling of an ophthalmic aneurysm.
Lessons: Several factors can precipitate intraoperative aneurysm rupture. Osmotic agents like mannitol can cause rapid intravascular fluid shifts, increasing hemodynamic stress across the aneurysm dome. Atmospheric pressure changes due to intraoperative manipulation can also alter extravascular forces on the aneurysm. Based on this experience, especially in young patients with prior unexplained hemorrhage, the authors advise careful use of mannitol and surgical technique. Surgeons should consider these risks in patients with known or suspected aneurysms to prevent catastrophic rupture. https://thejns.org/doi/10.3171/CASE25431.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


