{"title":"垂体腺瘤手术后的综合生育管理:日本农村病例的经验教训及实践回顾。","authors":"Daisuke Numahata, Kosuke Kojo, San-E Ishikawa, Takumi Kuramae, Ayumi Nakazono, Kaoru Yanagida, Hiroyuki Nishiyama, Tatsuya Takayama","doi":"10.3390/reports8030144","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background and Clinical Significance:</b> Pituitary adenomas, also termed pituitary neuroendocrine tumors, pose a significant risk of hypogonadotropic hypogonadism (HH) after surgical resection, with profound consequences for fertility and sexual function in young patients. <b>Case Presentation:</b> We present the case of a 29-year-old man from rural Japan who developed severe HH and azoospermia following two transsphenoidal resections for a large pituitary adenoma. Despite early engagement with neurosurgery teams, fertility management was delayed by the absence of on-site endocrinology expertise and limited local oncofertility resources. After comprehensive endocrine evaluation and counseling, the patient began combined human chorionic gonadotropin and recombinant follicle-stimulating hormone therapy, resulting in full recovery of sexual function and normalization of semen parameters, ultimately leading to spontaneous conception and the birth of a healthy child. Building on this real-world case, we provide a narrative review of current practical management strategies for HH after pituitary surgery, including the utility of hormone-stimulation tests, Japanese guideline-based subsidy systems, and best-practice approaches to hormonal replacement. <b>Conclusions:</b> This case underscores not only the necessity for early, interdisciplinary collaboration and preoperative counseling but also highlights a rare instance in which a patient with a benign tumor received care that did not address his fertility-related needs, emphasizing that such considerations should be integrated into preoperative counseling even for non-malignant conditions. Strengthening regional oncofertility networks and improving healthcare providers' awareness of fertility-preservation options remain essential for improving outcomes.</p>","PeriodicalId":74664,"journal":{"name":"Reports (MDPI)","volume":"8 3","pages":""},"PeriodicalIF":0.8000,"publicationDate":"2025-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12371999/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comprehensive Fertility Management After Pituitary Adenoma Surgery: Lessons from a Rural Japanese Case and Practical Review.\",\"authors\":\"Daisuke Numahata, Kosuke Kojo, San-E Ishikawa, Takumi Kuramae, Ayumi Nakazono, Kaoru Yanagida, Hiroyuki Nishiyama, Tatsuya Takayama\",\"doi\":\"10.3390/reports8030144\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background and Clinical Significance:</b> Pituitary adenomas, also termed pituitary neuroendocrine tumors, pose a significant risk of hypogonadotropic hypogonadism (HH) after surgical resection, with profound consequences for fertility and sexual function in young patients. <b>Case Presentation:</b> We present the case of a 29-year-old man from rural Japan who developed severe HH and azoospermia following two transsphenoidal resections for a large pituitary adenoma. Despite early engagement with neurosurgery teams, fertility management was delayed by the absence of on-site endocrinology expertise and limited local oncofertility resources. After comprehensive endocrine evaluation and counseling, the patient began combined human chorionic gonadotropin and recombinant follicle-stimulating hormone therapy, resulting in full recovery of sexual function and normalization of semen parameters, ultimately leading to spontaneous conception and the birth of a healthy child. Building on this real-world case, we provide a narrative review of current practical management strategies for HH after pituitary surgery, including the utility of hormone-stimulation tests, Japanese guideline-based subsidy systems, and best-practice approaches to hormonal replacement. <b>Conclusions:</b> This case underscores not only the necessity for early, interdisciplinary collaboration and preoperative counseling but also highlights a rare instance in which a patient with a benign tumor received care that did not address his fertility-related needs, emphasizing that such considerations should be integrated into preoperative counseling even for non-malignant conditions. Strengthening regional oncofertility networks and improving healthcare providers' awareness of fertility-preservation options remain essential for improving outcomes.</p>\",\"PeriodicalId\":74664,\"journal\":{\"name\":\"Reports (MDPI)\",\"volume\":\"8 3\",\"pages\":\"\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2025-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12371999/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Reports (MDPI)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/reports8030144\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Reports (MDPI)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/reports8030144","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Comprehensive Fertility Management After Pituitary Adenoma Surgery: Lessons from a Rural Japanese Case and Practical Review.
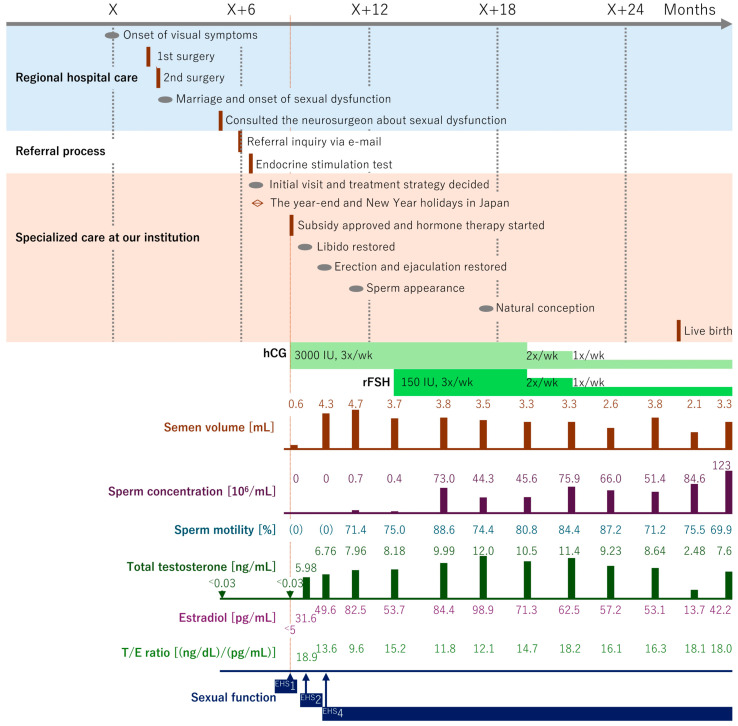
Background and Clinical Significance: Pituitary adenomas, also termed pituitary neuroendocrine tumors, pose a significant risk of hypogonadotropic hypogonadism (HH) after surgical resection, with profound consequences for fertility and sexual function in young patients. Case Presentation: We present the case of a 29-year-old man from rural Japan who developed severe HH and azoospermia following two transsphenoidal resections for a large pituitary adenoma. Despite early engagement with neurosurgery teams, fertility management was delayed by the absence of on-site endocrinology expertise and limited local oncofertility resources. After comprehensive endocrine evaluation and counseling, the patient began combined human chorionic gonadotropin and recombinant follicle-stimulating hormone therapy, resulting in full recovery of sexual function and normalization of semen parameters, ultimately leading to spontaneous conception and the birth of a healthy child. Building on this real-world case, we provide a narrative review of current practical management strategies for HH after pituitary surgery, including the utility of hormone-stimulation tests, Japanese guideline-based subsidy systems, and best-practice approaches to hormonal replacement. Conclusions: This case underscores not only the necessity for early, interdisciplinary collaboration and preoperative counseling but also highlights a rare instance in which a patient with a benign tumor received care that did not address his fertility-related needs, emphasizing that such considerations should be integrated into preoperative counseling even for non-malignant conditions. Strengthening regional oncofertility networks and improving healthcare providers' awareness of fertility-preservation options remain essential for improving outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


