Yeung-Ae Park, Anya Kitt Lee, Rahul D Barmanray, Frank Gao, Spiros Fourlanos, Chris Gilfillan
{"title":"服用和不服用SGLT2抑制剂的患者使用DKA和胰岛素的持续时间","authors":"Yeung-Ae Park, Anya Kitt Lee, Rahul D Barmanray, Frank Gao, Spiros Fourlanos, Chris Gilfillan","doi":"10.3390/medicines12030021","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/objectives: </strong>Sodium-glucose co-transporter 2 inhibitors (SGLT2i) are associated with increased rates of diabetic ketoacidosis (DKA). The difference in the management and outcomes of SGLT2i-associated DKA (SGLT2i DKA) from non-SGLT2i-associated DKA (non-SGLT2i DKA) remains unclear due to a lack of specific reporting on dextrose and insulin. This study aims to compare the management and outcome of SGLT2i and non-SGLT2i diabetic ketoacidosis.</p><p><strong>Methods: </strong>In this retrospective cohort study, patients admitted to the Intensive Care Unit (ICU) for diabetic ketosis between 1 January 2020 to 31 December 2021 at a tertiary hospital were identified. For each SGLT2i diabetic ketosis, two non-SGLT2i diabetic ketosis admissions closest to the SGLT2i admission date were evaluated for comparison. Clinical data including biochemistry, ICU length of stay (LOS), time to normalize acidemia and ketonemia, dextrose and insulin requirements, were evaluated.</p><p><strong>Results: </strong>In the SGLT2i group (<i>n</i> = 30), there were 22 DKA and 8 diabetic ketosis cases; in the non-SGLT2i group (<i>n</i> = 60), there were 54 DKA and 6 diabetic ketosis cases. SGLT2i DKA (<i>n</i> = 22) required 62% greater total insulin (154 [117-249] vs. 95 [59-150] units; <i>p</i> = 0.004), which remained statistically significant after weight adjustment (<i>p</i> = 0.02), and longer ICU LOS (52 [42-97] vs. 39 [23-68] hours; <i>p</i> = 0.01) compared to non-SGLT2i DKA (<i>n</i> = 54), despite a comparable time to DKA resolution (22 [15-35] vs. 20 [15-35] hours; <i>p</i> = 0.91). In the intercurrent illness subgroup analysis, neither total insulin dose nor ICU LOS remained statistically significantly different between SGLT2i (<i>n</i> = 16) and non-SGLT2i DKA (<i>n</i> = 21). The majority of cases received 10% dextrose and variable rate intravenous insulin infusion (VRIII).</p><p><strong>Conclusions: </strong>The greater insulin requirement in SGLT2i DKA compared to non-SGLT2i DKA may be explained by the greater proportion of precipitating intercurrent illnesses and demographic differences in SGLT2i DKA, highlighting that SGLT2i DKA (predominantly comprising T2D) and non-SGLT2i DKA (predominantly comprising T1D) represent distinct clinical entities. Our findings in comparison to the literature imply that in SGLT2i DKA, the need for prolonged IV insulin infusion may be reduced through intensive management using intravenous 10% dextrose and VRIII. Prospective studies are warranted to evaluate the efficacy of different management strategies for SGLT2i DKA.</p>","PeriodicalId":74162,"journal":{"name":"Medicines (Basel, Switzerland)","volume":"12 3","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12371971/pdf/","citationCount":"0","resultStr":"{\"title\":\"Duration of DKA and Insulin Use in People with and Without SGLT2 Inhibitor Medications.\",\"authors\":\"Yeung-Ae Park, Anya Kitt Lee, Rahul D Barmanray, Frank Gao, Spiros Fourlanos, Chris Gilfillan\",\"doi\":\"10.3390/medicines12030021\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background/objectives: </strong>Sodium-glucose co-transporter 2 inhibitors (SGLT2i) are associated with increased rates of diabetic ketoacidosis (DKA). The difference in the management and outcomes of SGLT2i-associated DKA (SGLT2i DKA) from non-SGLT2i-associated DKA (non-SGLT2i DKA) remains unclear due to a lack of specific reporting on dextrose and insulin. This study aims to compare the management and outcome of SGLT2i and non-SGLT2i diabetic ketoacidosis.</p><p><strong>Methods: </strong>In this retrospective cohort study, patients admitted to the Intensive Care Unit (ICU) for diabetic ketosis between 1 January 2020 to 31 December 2021 at a tertiary hospital were identified. For each SGLT2i diabetic ketosis, two non-SGLT2i diabetic ketosis admissions closest to the SGLT2i admission date were evaluated for comparison. Clinical data including biochemistry, ICU length of stay (LOS), time to normalize acidemia and ketonemia, dextrose and insulin requirements, were evaluated.</p><p><strong>Results: </strong>In the SGLT2i group (<i>n</i> = 30), there were 22 DKA and 8 diabetic ketosis cases; in the non-SGLT2i group (<i>n</i> = 60), there were 54 DKA and 6 diabetic ketosis cases. SGLT2i DKA (<i>n</i> = 22) required 62% greater total insulin (154 [117-249] vs. 95 [59-150] units; <i>p</i> = 0.004), which remained statistically significant after weight adjustment (<i>p</i> = 0.02), and longer ICU LOS (52 [42-97] vs. 39 [23-68] hours; <i>p</i> = 0.01) compared to non-SGLT2i DKA (<i>n</i> = 54), despite a comparable time to DKA resolution (22 [15-35] vs. 20 [15-35] hours; <i>p</i> = 0.91). In the intercurrent illness subgroup analysis, neither total insulin dose nor ICU LOS remained statistically significantly different between SGLT2i (<i>n</i> = 16) and non-SGLT2i DKA (<i>n</i> = 21). The majority of cases received 10% dextrose and variable rate intravenous insulin infusion (VRIII).</p><p><strong>Conclusions: </strong>The greater insulin requirement in SGLT2i DKA compared to non-SGLT2i DKA may be explained by the greater proportion of precipitating intercurrent illnesses and demographic differences in SGLT2i DKA, highlighting that SGLT2i DKA (predominantly comprising T2D) and non-SGLT2i DKA (predominantly comprising T1D) represent distinct clinical entities. Our findings in comparison to the literature imply that in SGLT2i DKA, the need for prolonged IV insulin infusion may be reduced through intensive management using intravenous 10% dextrose and VRIII. Prospective studies are warranted to evaluate the efficacy of different management strategies for SGLT2i DKA.</p>\",\"PeriodicalId\":74162,\"journal\":{\"name\":\"Medicines (Basel, Switzerland)\",\"volume\":\"12 3\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12371971/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Medicines (Basel, Switzerland)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/medicines12030021\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Medicines (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/medicines12030021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Duration of DKA and Insulin Use in People with and Without SGLT2 Inhibitor Medications.
Background/objectives: Sodium-glucose co-transporter 2 inhibitors (SGLT2i) are associated with increased rates of diabetic ketoacidosis (DKA). The difference in the management and outcomes of SGLT2i-associated DKA (SGLT2i DKA) from non-SGLT2i-associated DKA (non-SGLT2i DKA) remains unclear due to a lack of specific reporting on dextrose and insulin. This study aims to compare the management and outcome of SGLT2i and non-SGLT2i diabetic ketoacidosis.
Methods: In this retrospective cohort study, patients admitted to the Intensive Care Unit (ICU) for diabetic ketosis between 1 January 2020 to 31 December 2021 at a tertiary hospital were identified. For each SGLT2i diabetic ketosis, two non-SGLT2i diabetic ketosis admissions closest to the SGLT2i admission date were evaluated for comparison. Clinical data including biochemistry, ICU length of stay (LOS), time to normalize acidemia and ketonemia, dextrose and insulin requirements, were evaluated.
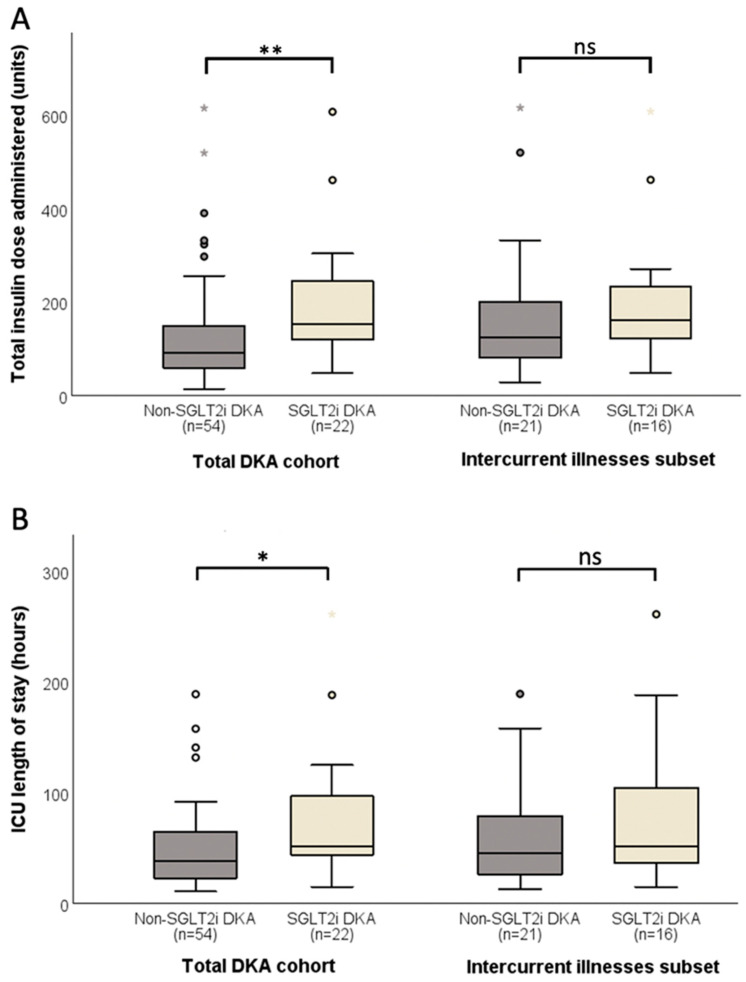
Results: In the SGLT2i group (n = 30), there were 22 DKA and 8 diabetic ketosis cases; in the non-SGLT2i group (n = 60), there were 54 DKA and 6 diabetic ketosis cases. SGLT2i DKA (n = 22) required 62% greater total insulin (154 [117-249] vs. 95 [59-150] units; p = 0.004), which remained statistically significant after weight adjustment (p = 0.02), and longer ICU LOS (52 [42-97] vs. 39 [23-68] hours; p = 0.01) compared to non-SGLT2i DKA (n = 54), despite a comparable time to DKA resolution (22 [15-35] vs. 20 [15-35] hours; p = 0.91). In the intercurrent illness subgroup analysis, neither total insulin dose nor ICU LOS remained statistically significantly different between SGLT2i (n = 16) and non-SGLT2i DKA (n = 21). The majority of cases received 10% dextrose and variable rate intravenous insulin infusion (VRIII).
Conclusions: The greater insulin requirement in SGLT2i DKA compared to non-SGLT2i DKA may be explained by the greater proportion of precipitating intercurrent illnesses and demographic differences in SGLT2i DKA, highlighting that SGLT2i DKA (predominantly comprising T2D) and non-SGLT2i DKA (predominantly comprising T1D) represent distinct clinical entities. Our findings in comparison to the literature imply that in SGLT2i DKA, the need for prolonged IV insulin infusion may be reduced through intensive management using intravenous 10% dextrose and VRIII. Prospective studies are warranted to evaluate the efficacy of different management strategies for SGLT2i DKA.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


