Brenna S Kincaid, Kiana Kim, Jennifer L Waller, Stephanie L Baer, Wendy B Bollag, Roni J Bollag
{"title":"血浆交换治疗的血栓性血小板减少性紫癜与终末期肾病患者死亡率改善的关系","authors":"Brenna S Kincaid, Kiana Kim, Jennifer L Waller, Stephanie L Baer, Wendy B Bollag, Roni J Bollag","doi":"10.3390/diseases13080247","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background/Objectives</b>: Thrombotic thrombocytopenic purpura (TTP) is a microangiopathic hemolytic anemia exhibiting 90% mortality without prompt treatment. The aim of this study was to investigate the association of therapeutic plasma exchange (TPE)-treated TTP in end-stage renal disease (ESRD) patients with mortality, demographics, and clinical comorbidities. We queried the United States Renal Data System for ESRD patients starting dialysis between 1 January 2005 and 31 December 2018, using International Classification of Diseases (ICD)-9 and ICD-10 codes for thrombotic microangiopathy, with a TPE procedure code entered within 7 days. <b>Methods</b>: Cox proportional hazards models were used to assess mortality, adjusting for demographic and clinical factors. <b>Results</b>: Among 1,155,136 patients, increased age [adjusted odds ratio (OR) = 0.96, 95% confidence interval (CI): 0.94-0.96]; black race (OR = 0.67, CI: 0.51-0.89); and Hispanic ethnicity (OR = 0.43, CI: 0.28-0.66) were associated with a lower risk of TPE-treated TTP diagnosis, whereas female sex (OR = 1.59, CI: 1.25-2.02) and tobacco use (OR = 2.08, CI: 1.58-2.75) had a higher risk. A claim for TPE-treated TTP carried a lower risk of death (adjusted hazard ratio = 0.024, CI: 0.021-0.028). Female sex, black race, Hispanic ethnicity, and hypothyroidism were also associated with decreased all-cause mortality. <b>Conclusions</b>: These findings suggest that ESRD patients with TPE-treated TTP are significantly protected from mortality compared with ESRD patients without this diagnosis.</p>","PeriodicalId":72832,"journal":{"name":"Diseases (Basel, Switzerland)","volume":"13 8","pages":""},"PeriodicalIF":3.0000,"publicationDate":"2025-08-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12385575/pdf/","citationCount":"0","resultStr":"{\"title\":\"Association of Therapeutic Plasma Exchange-Treated Thrombotic Thrombocytopenic Purpura with Improved Mortality Outcome in End-Stage Renal Disease.\",\"authors\":\"Brenna S Kincaid, Kiana Kim, Jennifer L Waller, Stephanie L Baer, Wendy B Bollag, Roni J Bollag\",\"doi\":\"10.3390/diseases13080247\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b>Background/Objectives</b>: Thrombotic thrombocytopenic purpura (TTP) is a microangiopathic hemolytic anemia exhibiting 90% mortality without prompt treatment. The aim of this study was to investigate the association of therapeutic plasma exchange (TPE)-treated TTP in end-stage renal disease (ESRD) patients with mortality, demographics, and clinical comorbidities. We queried the United States Renal Data System for ESRD patients starting dialysis between 1 January 2005 and 31 December 2018, using International Classification of Diseases (ICD)-9 and ICD-10 codes for thrombotic microangiopathy, with a TPE procedure code entered within 7 days. <b>Methods</b>: Cox proportional hazards models were used to assess mortality, adjusting for demographic and clinical factors. <b>Results</b>: Among 1,155,136 patients, increased age [adjusted odds ratio (OR) = 0.96, 95% confidence interval (CI): 0.94-0.96]; black race (OR = 0.67, CI: 0.51-0.89); and Hispanic ethnicity (OR = 0.43, CI: 0.28-0.66) were associated with a lower risk of TPE-treated TTP diagnosis, whereas female sex (OR = 1.59, CI: 1.25-2.02) and tobacco use (OR = 2.08, CI: 1.58-2.75) had a higher risk. A claim for TPE-treated TTP carried a lower risk of death (adjusted hazard ratio = 0.024, CI: 0.021-0.028). Female sex, black race, Hispanic ethnicity, and hypothyroidism were also associated with decreased all-cause mortality. <b>Conclusions</b>: These findings suggest that ESRD patients with TPE-treated TTP are significantly protected from mortality compared with ESRD patients without this diagnosis.</p>\",\"PeriodicalId\":72832,\"journal\":{\"name\":\"Diseases (Basel, Switzerland)\",\"volume\":\"13 8\",\"pages\":\"\"},\"PeriodicalIF\":3.0000,\"publicationDate\":\"2025-08-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12385575/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diseases (Basel, Switzerland)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3390/diseases13080247\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diseases (Basel, Switzerland)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3390/diseases13080247","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Association of Therapeutic Plasma Exchange-Treated Thrombotic Thrombocytopenic Purpura with Improved Mortality Outcome in End-Stage Renal Disease.
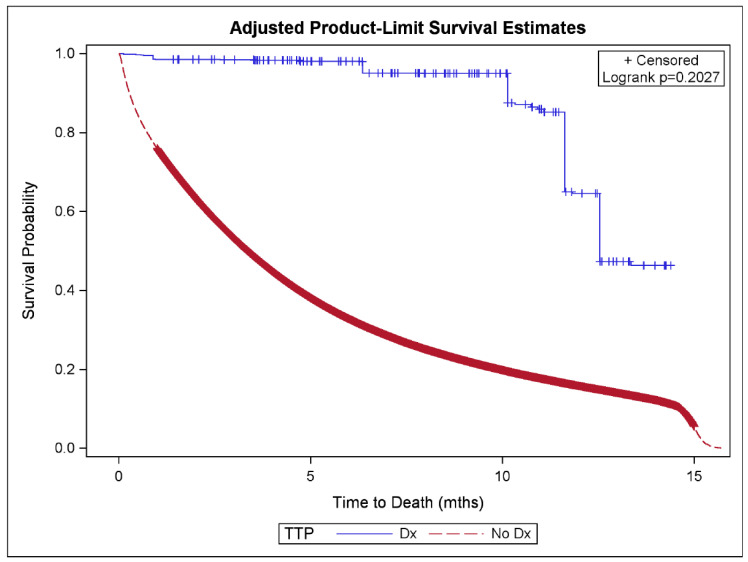
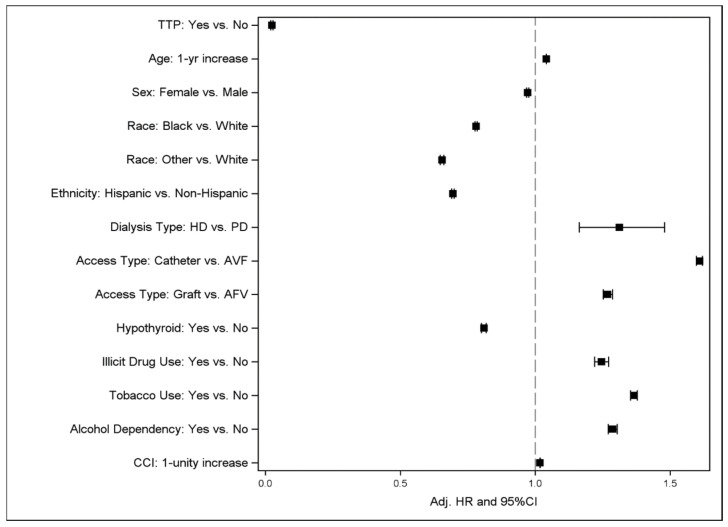
Background/Objectives: Thrombotic thrombocytopenic purpura (TTP) is a microangiopathic hemolytic anemia exhibiting 90% mortality without prompt treatment. The aim of this study was to investigate the association of therapeutic plasma exchange (TPE)-treated TTP in end-stage renal disease (ESRD) patients with mortality, demographics, and clinical comorbidities. We queried the United States Renal Data System for ESRD patients starting dialysis between 1 January 2005 and 31 December 2018, using International Classification of Diseases (ICD)-9 and ICD-10 codes for thrombotic microangiopathy, with a TPE procedure code entered within 7 days. Methods: Cox proportional hazards models were used to assess mortality, adjusting for demographic and clinical factors. Results: Among 1,155,136 patients, increased age [adjusted odds ratio (OR) = 0.96, 95% confidence interval (CI): 0.94-0.96]; black race (OR = 0.67, CI: 0.51-0.89); and Hispanic ethnicity (OR = 0.43, CI: 0.28-0.66) were associated with a lower risk of TPE-treated TTP diagnosis, whereas female sex (OR = 1.59, CI: 1.25-2.02) and tobacco use (OR = 2.08, CI: 1.58-2.75) had a higher risk. A claim for TPE-treated TTP carried a lower risk of death (adjusted hazard ratio = 0.024, CI: 0.021-0.028). Female sex, black race, Hispanic ethnicity, and hypothyroidism were also associated with decreased all-cause mortality. Conclusions: These findings suggest that ESRD patients with TPE-treated TTP are significantly protected from mortality compared with ESRD patients without this diagnosis.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


