Amalie D Haue, Peter C Holm, Karina Banasik, Kenny Emil Aunstrup, Christian Holm Johansen, Agnete T Lundgaard, Victorine P Muse, Timo Röder, David Westergaard, Piotr J Chmura, Alex H Christensen, Peter E Weeke, Erik Sørensen, Ole B V Pedersen, Sisse R Ostrowski, Kasper K Iversen, Lars V Køber, Henrik Ullum, Henning Bundgaard, Søren Brunak
{"title":"用马尔可夫聚类算法对缺血性心脏病患者进行亚组。","authors":"Amalie D Haue, Peter C Holm, Karina Banasik, Kenny Emil Aunstrup, Christian Holm Johansen, Agnete T Lundgaard, Victorine P Muse, Timo Röder, David Westergaard, Piotr J Chmura, Alex H Christensen, Peter E Weeke, Erik Sørensen, Ole B V Pedersen, Sisse R Ostrowski, Kasper K Iversen, Lars V Køber, Henrik Ullum, Henning Bundgaard, Søren Brunak","doi":"10.1038/s43856-025-01077-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Ischemic heart disease (IHD) is heterogeneous with respect to onset, burden of symptoms, and disease progression. We hypothesized that unsupervised clustering analysis could facilitate identification of distinct and clinically relevant multimorbidity clusters.</p><p><strong>Methods: </strong>We included IHD patients who underwent coronary angiography (CAG) or coronary computed tomography angiography (CCTA) between 2004 and 2016 and used the earliest procedure as the index date. Patient health records were obtained from the Danish National Patient Registry, the Danish National Prescription Registry, and two in-hospital laboratory database systems. Genetic data were obtained from the Copenhagen Hospital Biobank. Using registered pre-index diagnosis codes (n = 3046), patients were clustered by application of the Markov Cluster algorithm. Multimorbidity clusters were then characterized using Cox regressions (new ischemic events, non-IHD mortality, and all-cause mortality) and enrichment analysis to explore both risks and phenotypical characteristics.</p><p><strong>Results: </strong>In a cohort of 72,249 patients with IHD (mean age 63.9 years, 63.1% males), 31 distinct clusters (C1-31, 67,136 patients) are identified. Comparing each cluster to the 30 others, seven clusters (9,590 patients) have significantly higher or lower risk of new ischemic events (five and two clusters, respectively). A total of 18 clusters (35,982 patients) have higher or lower risk of death from non-IHD causes (12 and six clusters, respectively), and 23 clusters have a statistically significant higher or lower risk for all-cause mortality. Cardiovascular or inflammatory diseases are commonly enriched in clusters (13). Distributions for 24 laboratory test results differ significantly across clusters. Polygenic risk scores are increased in a total of 15 clusters (48.4%).</p><p><strong>Conclusions: </strong>Based on prior disease profiles, unsupervised clustering robustly stratify patients with IHD in subgroups with similar clinical features and outcomes.</p>","PeriodicalId":72646,"journal":{"name":"Communications medicine","volume":"5 1","pages":"372"},"PeriodicalIF":5.4000,"publicationDate":"2025-08-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12381225/pdf/","citationCount":"0","resultStr":"{\"title\":\"Subgrouping patients with ischemic heart disease by means of the Markov cluster algorithm.\",\"authors\":\"Amalie D Haue, Peter C Holm, Karina Banasik, Kenny Emil Aunstrup, Christian Holm Johansen, Agnete T Lundgaard, Victorine P Muse, Timo Röder, David Westergaard, Piotr J Chmura, Alex H Christensen, Peter E Weeke, Erik Sørensen, Ole B V Pedersen, Sisse R Ostrowski, Kasper K Iversen, Lars V Køber, Henrik Ullum, Henning Bundgaard, Søren Brunak\",\"doi\":\"10.1038/s43856-025-01077-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Ischemic heart disease (IHD) is heterogeneous with respect to onset, burden of symptoms, and disease progression. We hypothesized that unsupervised clustering analysis could facilitate identification of distinct and clinically relevant multimorbidity clusters.</p><p><strong>Methods: </strong>We included IHD patients who underwent coronary angiography (CAG) or coronary computed tomography angiography (CCTA) between 2004 and 2016 and used the earliest procedure as the index date. Patient health records were obtained from the Danish National Patient Registry, the Danish National Prescription Registry, and two in-hospital laboratory database systems. Genetic data were obtained from the Copenhagen Hospital Biobank. Using registered pre-index diagnosis codes (n = 3046), patients were clustered by application of the Markov Cluster algorithm. Multimorbidity clusters were then characterized using Cox regressions (new ischemic events, non-IHD mortality, and all-cause mortality) and enrichment analysis to explore both risks and phenotypical characteristics.</p><p><strong>Results: </strong>In a cohort of 72,249 patients with IHD (mean age 63.9 years, 63.1% males), 31 distinct clusters (C1-31, 67,136 patients) are identified. Comparing each cluster to the 30 others, seven clusters (9,590 patients) have significantly higher or lower risk of new ischemic events (five and two clusters, respectively). A total of 18 clusters (35,982 patients) have higher or lower risk of death from non-IHD causes (12 and six clusters, respectively), and 23 clusters have a statistically significant higher or lower risk for all-cause mortality. Cardiovascular or inflammatory diseases are commonly enriched in clusters (13). Distributions for 24 laboratory test results differ significantly across clusters. Polygenic risk scores are increased in a total of 15 clusters (48.4%).</p><p><strong>Conclusions: </strong>Based on prior disease profiles, unsupervised clustering robustly stratify patients with IHD in subgroups with similar clinical features and outcomes.</p>\",\"PeriodicalId\":72646,\"journal\":{\"name\":\"Communications medicine\",\"volume\":\"5 1\",\"pages\":\"372\"},\"PeriodicalIF\":5.4000,\"publicationDate\":\"2025-08-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12381225/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Communications medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1038/s43856-025-01077-1\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"MEDICINE, RESEARCH & EXPERIMENTAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Communications medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1038/s43856-025-01077-1","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
Subgrouping patients with ischemic heart disease by means of the Markov cluster algorithm.
Background: Ischemic heart disease (IHD) is heterogeneous with respect to onset, burden of symptoms, and disease progression. We hypothesized that unsupervised clustering analysis could facilitate identification of distinct and clinically relevant multimorbidity clusters.
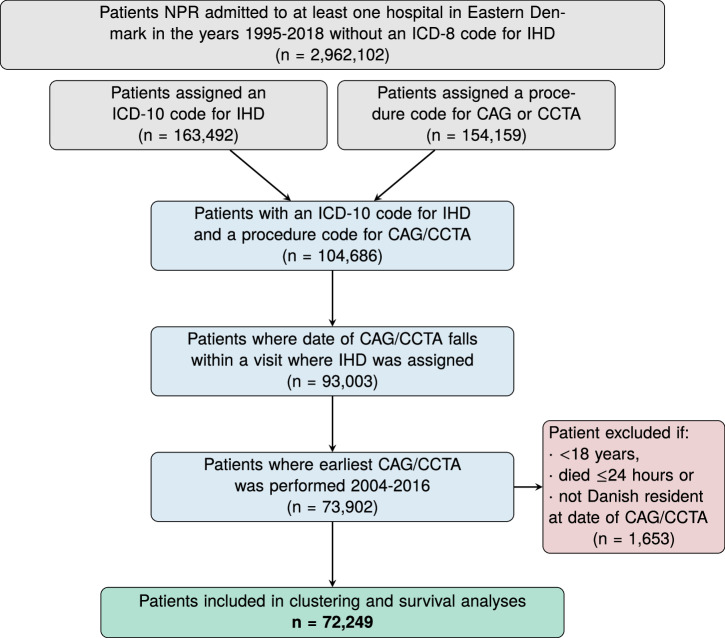
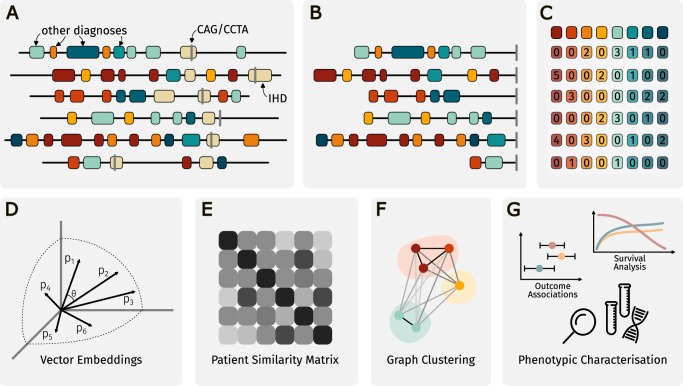
Methods: We included IHD patients who underwent coronary angiography (CAG) or coronary computed tomography angiography (CCTA) between 2004 and 2016 and used the earliest procedure as the index date. Patient health records were obtained from the Danish National Patient Registry, the Danish National Prescription Registry, and two in-hospital laboratory database systems. Genetic data were obtained from the Copenhagen Hospital Biobank. Using registered pre-index diagnosis codes (n = 3046), patients were clustered by application of the Markov Cluster algorithm. Multimorbidity clusters were then characterized using Cox regressions (new ischemic events, non-IHD mortality, and all-cause mortality) and enrichment analysis to explore both risks and phenotypical characteristics.
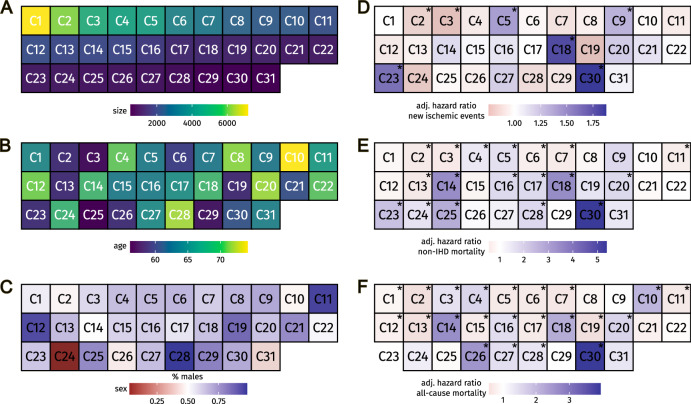
Results: In a cohort of 72,249 patients with IHD (mean age 63.9 years, 63.1% males), 31 distinct clusters (C1-31, 67,136 patients) are identified. Comparing each cluster to the 30 others, seven clusters (9,590 patients) have significantly higher or lower risk of new ischemic events (five and two clusters, respectively). A total of 18 clusters (35,982 patients) have higher or lower risk of death from non-IHD causes (12 and six clusters, respectively), and 23 clusters have a statistically significant higher or lower risk for all-cause mortality. Cardiovascular or inflammatory diseases are commonly enriched in clusters (13). Distributions for 24 laboratory test results differ significantly across clusters. Polygenic risk scores are increased in a total of 15 clusters (48.4%).
Conclusions: Based on prior disease profiles, unsupervised clustering robustly stratify patients with IHD in subgroups with similar clinical features and outcomes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


