Tomefa E Asempa, Tyler Ackley, Kristin E Linder, Cara D Riddle, Eric Walsh, David P Nicolau
{"title":"一项针对门诊诊所和急救中心社区获得性细菌性肺炎(CABP)的抗生素管理倡议:2023-2024年社区卫生系统经验","authors":"Tomefa E Asempa, Tyler Ackley, Kristin E Linder, Cara D Riddle, Eric Walsh, David P Nicolau","doi":"10.1017/ash.2025.10100","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This before-after study aimed to evaluate whether an order-set intervention would improve CABP-guideline concordance among outpatients.</p><p><strong>Setting: </strong>This study included adult patients presenting to outpatient clinics (<i>n</i> = 92) and urgent care centers (<i>n</i> = 39) within a community-based health system without a formal outpatient antibiotic stewardship program (ASP).</p><p><strong>Intervention: </strong>The intervention consisted of an antibiotic order-set and awareness campaign. Patient encounters were identified via CABP ICD-10 codes and IDSA-relevant patient comorbidities (chronic heart, lung, liver, or renal disease; diabetes mellitus; alcoholism; malignancy; asplenia) were extracted from the electronic health record. Primary outcome was to describe the proportion of patients receiving concordant therapy per IDSA guideline and local antibiogram in a pre- (May 2023 - April 2024) and post-intervention period (May 2024 - December 2024).</p><p><strong>Results: </strong>Baseline and intervention antibiotic concordance rate was 33.3% (1,467/4,401 encounters) and 28.0% (1,388/4,954 encounters), respectively. Among patients with no comorbidity, monotherapy prescriptions (concordant and discordant) decreased post-intervention and were replaced by higher levels of combination therapy (15% increase), albeit all discordant due to lack of comorbidities. Among patients with comorbidities, combination antibiotics increased by 12% post-intervention, driven by concordant prescriptions including amoxicillin/clavulanate plus azithromycin while the most frequently prescribed discordant combination was amoxicillin plus azithromycin. Trends were similar in primary care and urgent care centers.</p><p><strong>Conclusions: </strong>A stewardship intervention, including an order-set and awareness campaign improved the selection of combination therapy for appropriate patients but did not improve overall guideline concordance. For health systems without a dedicated outpatient ASP, these data will help bolster stewardship efforts towards more effective strategies.</p>","PeriodicalId":72246,"journal":{"name":"Antimicrobial stewardship & healthcare epidemiology : ASHE","volume":"5 1","pages":"e185"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394021/pdf/","citationCount":"0","resultStr":"{\"title\":\"An antibiotic stewardship initiative focused on community-acquired bacterial pneumonia (CABP) in outpatient clinics and urgent care centers: a 2023-2024 community health system experience.\",\"authors\":\"Tomefa E Asempa, Tyler Ackley, Kristin E Linder, Cara D Riddle, Eric Walsh, David P Nicolau\",\"doi\":\"10.1017/ash.2025.10100\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>This before-after study aimed to evaluate whether an order-set intervention would improve CABP-guideline concordance among outpatients.</p><p><strong>Setting: </strong>This study included adult patients presenting to outpatient clinics (<i>n</i> = 92) and urgent care centers (<i>n</i> = 39) within a community-based health system without a formal outpatient antibiotic stewardship program (ASP).</p><p><strong>Intervention: </strong>The intervention consisted of an antibiotic order-set and awareness campaign. Patient encounters were identified via CABP ICD-10 codes and IDSA-relevant patient comorbidities (chronic heart, lung, liver, or renal disease; diabetes mellitus; alcoholism; malignancy; asplenia) were extracted from the electronic health record. Primary outcome was to describe the proportion of patients receiving concordant therapy per IDSA guideline and local antibiogram in a pre- (May 2023 - April 2024) and post-intervention period (May 2024 - December 2024).</p><p><strong>Results: </strong>Baseline and intervention antibiotic concordance rate was 33.3% (1,467/4,401 encounters) and 28.0% (1,388/4,954 encounters), respectively. Among patients with no comorbidity, monotherapy prescriptions (concordant and discordant) decreased post-intervention and were replaced by higher levels of combination therapy (15% increase), albeit all discordant due to lack of comorbidities. Among patients with comorbidities, combination antibiotics increased by 12% post-intervention, driven by concordant prescriptions including amoxicillin/clavulanate plus azithromycin while the most frequently prescribed discordant combination was amoxicillin plus azithromycin. Trends were similar in primary care and urgent care centers.</p><p><strong>Conclusions: </strong>A stewardship intervention, including an order-set and awareness campaign improved the selection of combination therapy for appropriate patients but did not improve overall guideline concordance. For health systems without a dedicated outpatient ASP, these data will help bolster stewardship efforts towards more effective strategies.</p>\",\"PeriodicalId\":72246,\"journal\":{\"name\":\"Antimicrobial stewardship & healthcare epidemiology : ASHE\",\"volume\":\"5 1\",\"pages\":\"e185\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12394021/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Antimicrobial stewardship & healthcare epidemiology : ASHE\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1017/ash.2025.10100\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Antimicrobial stewardship & healthcare epidemiology : ASHE","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1017/ash.2025.10100","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
An antibiotic stewardship initiative focused on community-acquired bacterial pneumonia (CABP) in outpatient clinics and urgent care centers: a 2023-2024 community health system experience.
Objective: This before-after study aimed to evaluate whether an order-set intervention would improve CABP-guideline concordance among outpatients.
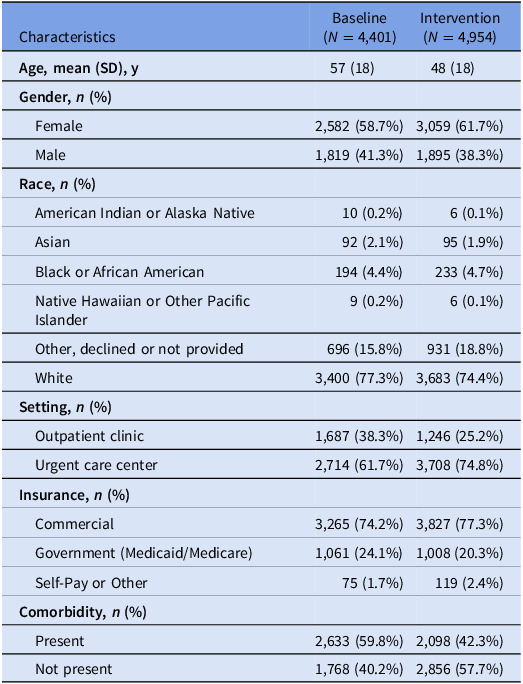
Setting: This study included adult patients presenting to outpatient clinics (n = 92) and urgent care centers (n = 39) within a community-based health system without a formal outpatient antibiotic stewardship program (ASP).
Intervention: The intervention consisted of an antibiotic order-set and awareness campaign. Patient encounters were identified via CABP ICD-10 codes and IDSA-relevant patient comorbidities (chronic heart, lung, liver, or renal disease; diabetes mellitus; alcoholism; malignancy; asplenia) were extracted from the electronic health record. Primary outcome was to describe the proportion of patients receiving concordant therapy per IDSA guideline and local antibiogram in a pre- (May 2023 - April 2024) and post-intervention period (May 2024 - December 2024).
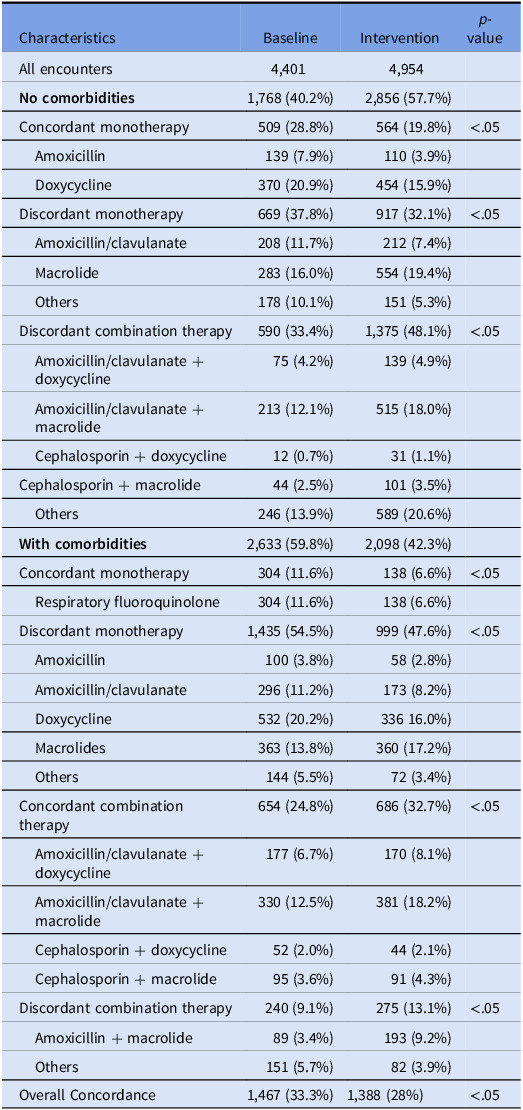
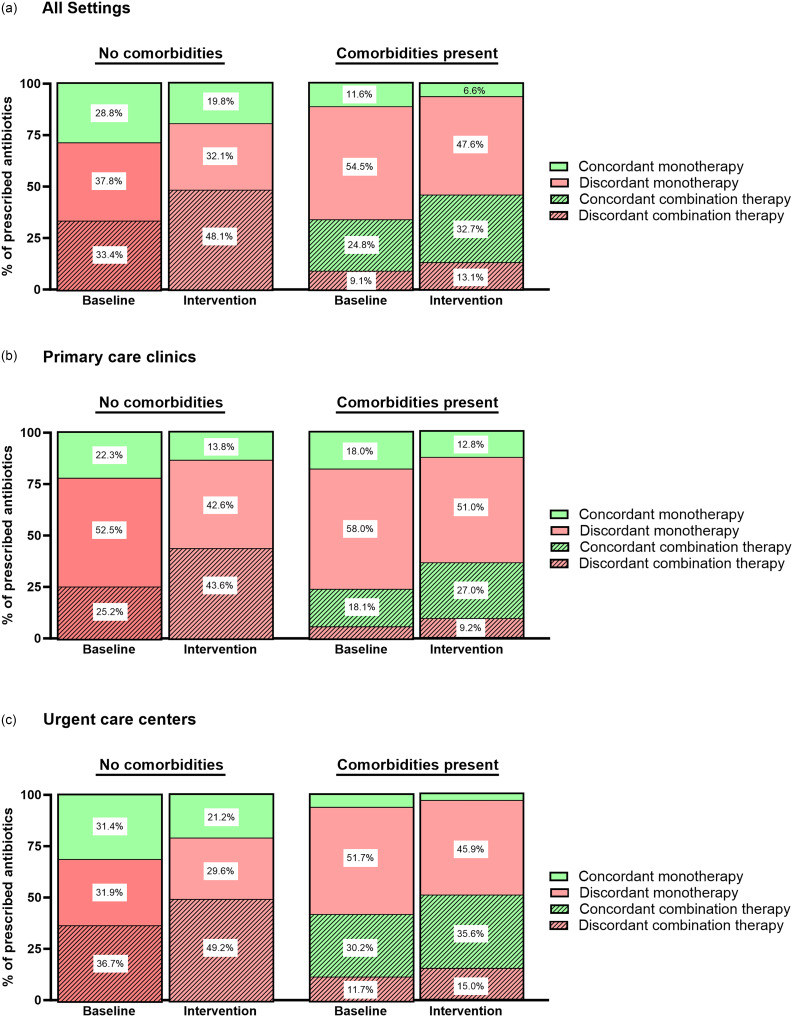
Results: Baseline and intervention antibiotic concordance rate was 33.3% (1,467/4,401 encounters) and 28.0% (1,388/4,954 encounters), respectively. Among patients with no comorbidity, monotherapy prescriptions (concordant and discordant) decreased post-intervention and were replaced by higher levels of combination therapy (15% increase), albeit all discordant due to lack of comorbidities. Among patients with comorbidities, combination antibiotics increased by 12% post-intervention, driven by concordant prescriptions including amoxicillin/clavulanate plus azithromycin while the most frequently prescribed discordant combination was amoxicillin plus azithromycin. Trends were similar in primary care and urgent care centers.
Conclusions: A stewardship intervention, including an order-set and awareness campaign improved the selection of combination therapy for appropriate patients but did not improve overall guideline concordance. For health systems without a dedicated outpatient ASP, these data will help bolster stewardship efforts towards more effective strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


