Wu Zeng, Gil Shapira, Tianjiao Gao, Michel Muvudi, Guohong Li, Jennifer Bouey, Delphin Antwisi, Fatma El Kadiri El Yamani
{"title":"对刚果民主共和国妇幼保健财政激励措施的经济评价:基于聚类随机对照试验的决策树模型","authors":"Wu Zeng, Gil Shapira, Tianjiao Gao, Michel Muvudi, Guohong Li, Jennifer Bouey, Delphin Antwisi, Fatma El Kadiri El Yamani","doi":"10.1186/s41256-025-00435-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>To improve the utilization of maternal and child health (MCH) services, the Democratic Republic of the Congo initiated a performance-based financing (PBF) program in 2017. An impact evaluation of the PBF program was conducted in 2023 using a cluster randomized controlled trial research design. This study aimed to assess the cost-effectiveness of the PBF program in comparison with the direct facility financing (DFF) program.</p><p><strong>Methods: </strong>A decision-tree model incorporating key MCH services was developed to estimate cost-effectiveness. Data on costs of maternal health services, epidemiological consequences, and utilities of various health statuses were obtained from the literature. The impact evaluation results on the coverage of key MCH services were included as key inputs to simulate the effectiveness measured as quality-adjusted life years (QALYs). Sensitivity analyses were conducted on the inclusion of the PBF's impact on the quality of care and the uncertainty regarding the costs and the impact of PBF on MCH services.</p><p><strong>Results: </strong>A total of US$205.9 million in 2021 dollar was spent on the PBF arm over the five years (2017-2021), with 70.60% allocated as incentive payments to health facilities and 19.41% as financial transfers to provincial purchasing agencies for contracting PBF facilities and managing the PBF program. On average, the annual cost per capita was estimated at US$2.05 and US$1.71 for implementing the PBF and DFF program, respectively. Without the quality adjustment, the improvement in MCH services resulted in 1,372 lives (192,036 QALYs) saved over 2017-2021. The incremental cost-effectiveness ratio (ICER) of the PBF program reached US$ 1,374 per QALY with substantial variation. After adjusting for quality, the ICER of PBF became smaller.</p><p><strong>Conclusions: </strong>Using three times the gross domestic product per capita in 2021 (US$1,732) as the threshold, the PBF program is a cost-effective strategy, though with substantial variation. It is crucial to take action to maintain gains from the improved MCH coverage resulting from the PBF program.</p>","PeriodicalId":52405,"journal":{"name":"Global Health Research and Policy","volume":"10 1","pages":"41"},"PeriodicalIF":4.6000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400745/pdf/","citationCount":"0","resultStr":"{\"title\":\"Economic evaluation of financial incentives for maternal and child health in the Democratic Republic of the Congo (DRC): a decision-tree modelling based on a cluster randomized controlled trial.\",\"authors\":\"Wu Zeng, Gil Shapira, Tianjiao Gao, Michel Muvudi, Guohong Li, Jennifer Bouey, Delphin Antwisi, Fatma El Kadiri El Yamani\",\"doi\":\"10.1186/s41256-025-00435-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>To improve the utilization of maternal and child health (MCH) services, the Democratic Republic of the Congo initiated a performance-based financing (PBF) program in 2017. An impact evaluation of the PBF program was conducted in 2023 using a cluster randomized controlled trial research design. This study aimed to assess the cost-effectiveness of the PBF program in comparison with the direct facility financing (DFF) program.</p><p><strong>Methods: </strong>A decision-tree model incorporating key MCH services was developed to estimate cost-effectiveness. Data on costs of maternal health services, epidemiological consequences, and utilities of various health statuses were obtained from the literature. The impact evaluation results on the coverage of key MCH services were included as key inputs to simulate the effectiveness measured as quality-adjusted life years (QALYs). Sensitivity analyses were conducted on the inclusion of the PBF's impact on the quality of care and the uncertainty regarding the costs and the impact of PBF on MCH services.</p><p><strong>Results: </strong>A total of US$205.9 million in 2021 dollar was spent on the PBF arm over the five years (2017-2021), with 70.60% allocated as incentive payments to health facilities and 19.41% as financial transfers to provincial purchasing agencies for contracting PBF facilities and managing the PBF program. On average, the annual cost per capita was estimated at US$2.05 and US$1.71 for implementing the PBF and DFF program, respectively. Without the quality adjustment, the improvement in MCH services resulted in 1,372 lives (192,036 QALYs) saved over 2017-2021. The incremental cost-effectiveness ratio (ICER) of the PBF program reached US$ 1,374 per QALY with substantial variation. After adjusting for quality, the ICER of PBF became smaller.</p><p><strong>Conclusions: </strong>Using three times the gross domestic product per capita in 2021 (US$1,732) as the threshold, the PBF program is a cost-effective strategy, though with substantial variation. It is crucial to take action to maintain gains from the improved MCH coverage resulting from the PBF program.</p>\",\"PeriodicalId\":52405,\"journal\":{\"name\":\"Global Health Research and Policy\",\"volume\":\"10 1\",\"pages\":\"41\"},\"PeriodicalIF\":4.6000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12400745/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Global Health Research and Policy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s41256-025-00435-9\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Global Health Research and Policy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s41256-025-00435-9","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
Economic evaluation of financial incentives for maternal and child health in the Democratic Republic of the Congo (DRC): a decision-tree modelling based on a cluster randomized controlled trial.
Background: To improve the utilization of maternal and child health (MCH) services, the Democratic Republic of the Congo initiated a performance-based financing (PBF) program in 2017. An impact evaluation of the PBF program was conducted in 2023 using a cluster randomized controlled trial research design. This study aimed to assess the cost-effectiveness of the PBF program in comparison with the direct facility financing (DFF) program.
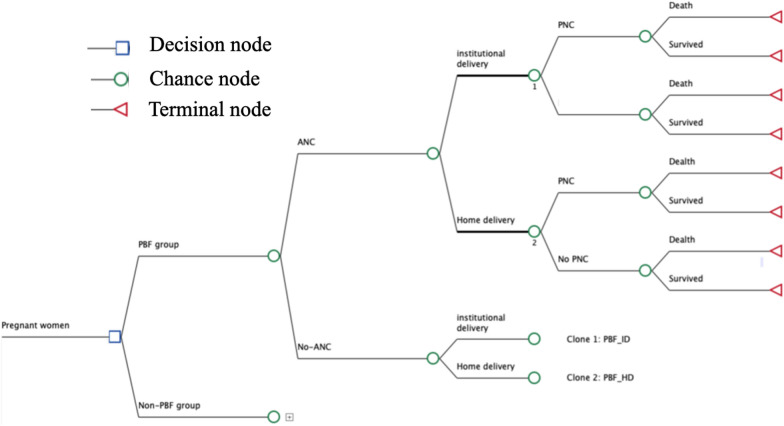
Methods: A decision-tree model incorporating key MCH services was developed to estimate cost-effectiveness. Data on costs of maternal health services, epidemiological consequences, and utilities of various health statuses were obtained from the literature. The impact evaluation results on the coverage of key MCH services were included as key inputs to simulate the effectiveness measured as quality-adjusted life years (QALYs). Sensitivity analyses were conducted on the inclusion of the PBF's impact on the quality of care and the uncertainty regarding the costs and the impact of PBF on MCH services.
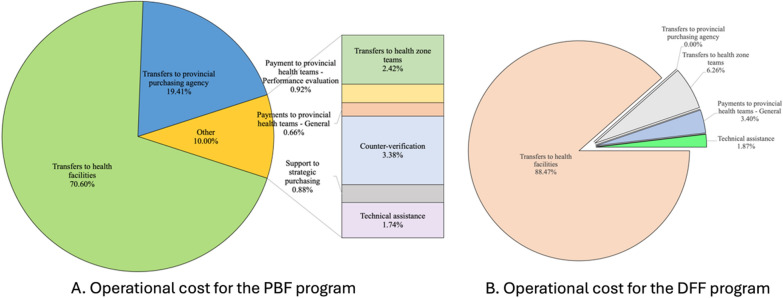
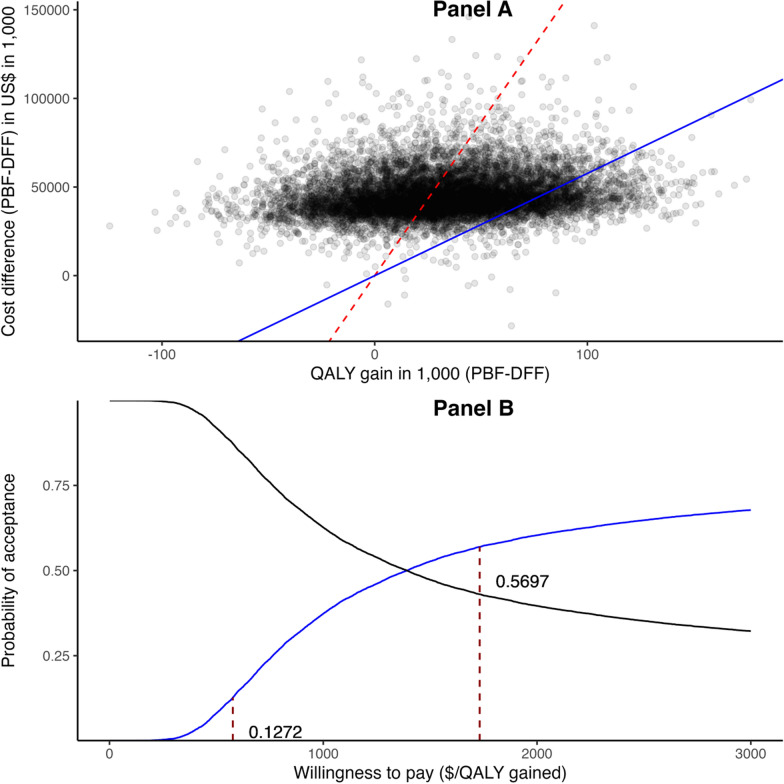
Results: A total of US$205.9 million in 2021 dollar was spent on the PBF arm over the five years (2017-2021), with 70.60% allocated as incentive payments to health facilities and 19.41% as financial transfers to provincial purchasing agencies for contracting PBF facilities and managing the PBF program. On average, the annual cost per capita was estimated at US$2.05 and US$1.71 for implementing the PBF and DFF program, respectively. Without the quality adjustment, the improvement in MCH services resulted in 1,372 lives (192,036 QALYs) saved over 2017-2021. The incremental cost-effectiveness ratio (ICER) of the PBF program reached US$ 1,374 per QALY with substantial variation. After adjusting for quality, the ICER of PBF became smaller.
Conclusions: Using three times the gross domestic product per capita in 2021 (US$1,732) as the threshold, the PBF program is a cost-effective strategy, though with substantial variation. It is crucial to take action to maintain gains from the improved MCH coverage resulting from the PBF program.
期刊介绍:
Global Health Research and Policy, an open-access, multidisciplinary journal, publishes research on various aspects of global health, addressing topics like health equity, health systems and policy, social determinants of health, disease burden, population health, and other urgent global health issues. It serves as a forum for high-quality research focused on regional and global health improvement, emphasizing solutions for health equity.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


