{"title":"成年女性原发性特发性乳糜心包。","authors":"Abdul Azeez Asad Mohammed, Hafsah Ali, Shaikh Swalehin Bux, Prashant Prabhakar, Abid Hussain, Waleed Dita","doi":"10.14797/mdcvj.1660","DOIUrl":null,"url":null,"abstract":"<p><p>Chylopericardium (CP), defined as the accumulation of chyle in the pericardial cavity, is a rare condition, especially in the absence of an identifiable secondary cause. Primary idiopathic chylopericardium (PIC) is even more uncommon, with limited cases reported in the literature. We report the case of a 43-year-old South Asian woman who presented with palpitations and fatigue. Echocardiography revealed a large pericardial effusion with signs of cardiac tamponade, necessitating emergent pericardiocentesis. The pericardial fluid aspirated was pinkish and turbid, which turned to milky white after centrifugation. Analysis of the pericardial fluid demonstrated a high triglyceride concentration, lymphocytic predominance, and fat globules, consistent with chylous effusion. A thorough diagnostic workup-including infectious, rheumatologic, and oncologic evaluations-was unrevealing, confirming a diagnosis of PIC. Lymphoscintigraphy was misleading in this case, with no thoracic duct abnormalities reported. Following an initial response to conservative management with pericardiocentesis and a medium-chain triglyceride-rich diet, the patient experienced recurrence of symptoms and fluid reaccumulation. Definitive management via thoracic duct ligation and pericardial window surgery was performed, resulting in complete resolution of the effusion. At 6-month follow-up, the patient remained asymptomatic with no evidence of recurrence. This case highlights the importance of considering primary CP in the differential diagnosis of pericardial effusion. Absence of classical inflammatory signs and symptoms can be suggestive of chylous effusion. The report also supports surgical intervention as a definitive treatment even if lymphoscintigraphy does not reveal clear thoracic duct pathology.</p>","PeriodicalId":39207,"journal":{"name":"Methodist DeBakey cardiovascular journal","volume":"21 1","pages":"84-89"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372655/pdf/","citationCount":"0","resultStr":"{\"title\":\"Primary Idiopathic Chylopericardium in an Adult Female.\",\"authors\":\"Abdul Azeez Asad Mohammed, Hafsah Ali, Shaikh Swalehin Bux, Prashant Prabhakar, Abid Hussain, Waleed Dita\",\"doi\":\"10.14797/mdcvj.1660\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Chylopericardium (CP), defined as the accumulation of chyle in the pericardial cavity, is a rare condition, especially in the absence of an identifiable secondary cause. Primary idiopathic chylopericardium (PIC) is even more uncommon, with limited cases reported in the literature. We report the case of a 43-year-old South Asian woman who presented with palpitations and fatigue. Echocardiography revealed a large pericardial effusion with signs of cardiac tamponade, necessitating emergent pericardiocentesis. The pericardial fluid aspirated was pinkish and turbid, which turned to milky white after centrifugation. Analysis of the pericardial fluid demonstrated a high triglyceride concentration, lymphocytic predominance, and fat globules, consistent with chylous effusion. A thorough diagnostic workup-including infectious, rheumatologic, and oncologic evaluations-was unrevealing, confirming a diagnosis of PIC. Lymphoscintigraphy was misleading in this case, with no thoracic duct abnormalities reported. Following an initial response to conservative management with pericardiocentesis and a medium-chain triglyceride-rich diet, the patient experienced recurrence of symptoms and fluid reaccumulation. Definitive management via thoracic duct ligation and pericardial window surgery was performed, resulting in complete resolution of the effusion. At 6-month follow-up, the patient remained asymptomatic with no evidence of recurrence. This case highlights the importance of considering primary CP in the differential diagnosis of pericardial effusion. Absence of classical inflammatory signs and symptoms can be suggestive of chylous effusion. The report also supports surgical intervention as a definitive treatment even if lymphoscintigraphy does not reveal clear thoracic duct pathology.</p>\",\"PeriodicalId\":39207,\"journal\":{\"name\":\"Methodist DeBakey cardiovascular journal\",\"volume\":\"21 1\",\"pages\":\"84-89\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12372655/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Methodist DeBakey cardiovascular journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14797/mdcvj.1660\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Methodist DeBakey cardiovascular journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14797/mdcvj.1660","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Primary Idiopathic Chylopericardium in an Adult Female.
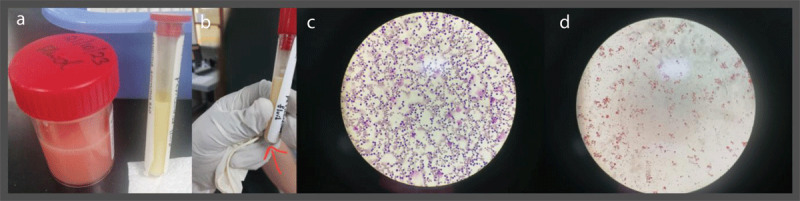
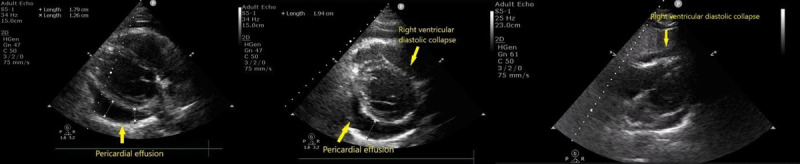
Chylopericardium (CP), defined as the accumulation of chyle in the pericardial cavity, is a rare condition, especially in the absence of an identifiable secondary cause. Primary idiopathic chylopericardium (PIC) is even more uncommon, with limited cases reported in the literature. We report the case of a 43-year-old South Asian woman who presented with palpitations and fatigue. Echocardiography revealed a large pericardial effusion with signs of cardiac tamponade, necessitating emergent pericardiocentesis. The pericardial fluid aspirated was pinkish and turbid, which turned to milky white after centrifugation. Analysis of the pericardial fluid demonstrated a high triglyceride concentration, lymphocytic predominance, and fat globules, consistent with chylous effusion. A thorough diagnostic workup-including infectious, rheumatologic, and oncologic evaluations-was unrevealing, confirming a diagnosis of PIC. Lymphoscintigraphy was misleading in this case, with no thoracic duct abnormalities reported. Following an initial response to conservative management with pericardiocentesis and a medium-chain triglyceride-rich diet, the patient experienced recurrence of symptoms and fluid reaccumulation. Definitive management via thoracic duct ligation and pericardial window surgery was performed, resulting in complete resolution of the effusion. At 6-month follow-up, the patient remained asymptomatic with no evidence of recurrence. This case highlights the importance of considering primary CP in the differential diagnosis of pericardial effusion. Absence of classical inflammatory signs and symptoms can be suggestive of chylous effusion. The report also supports surgical intervention as a definitive treatment even if lymphoscintigraphy does not reveal clear thoracic duct pathology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


