Aaron Saxton, David Song, Christopher Wanderling, Austin Lee, Timothy Campbell, Stephen Hassig, Yeon Joo Lee-Saxton, Sarah Jaffe, Kaitlyn Mitchell, Shlomi Tapiero, Rajat Jain, Scott O Quarrier
{"title":"减少疼痛和阿片类药物的使用:采用竖脊肌平面阻滞的经皮肾镜取石术的增强恢复途径的实施。","authors":"Aaron Saxton, David Song, Christopher Wanderling, Austin Lee, Timothy Campbell, Stephen Hassig, Yeon Joo Lee-Saxton, Sarah Jaffe, Kaitlyn Mitchell, Shlomi Tapiero, Rajat Jain, Scott O Quarrier","doi":"10.1097/CU9.0000000000000283","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>There is no standard analgesic pathway after percutaneous nephrolithotomy. At our institution, an Enhanced Recovery After Surgery (ERAS) pathway was instated that included a preoperative erector spinae plane (ESP) block to improve pain control and minimize opioid usage in the postoperative setting.</p><p><strong>Materials and methods: </strong>At our institution, an ERAS pathway was created for patients undergoing percutaneous nephrolithotomy. This pathway involved a preoperative ESP block and the replacement of opioids with multimodal analgesia. Patient charts were retrospectively reviewed and placed into 2 cohorts: one cohort participated in the ERAS pathway, whereas the other received traditional pain control. The primary outcome evaluated was postoperative morphine equivalents received. Secondary outcomes included nursing pain scores, opioid prescriptions for home, and quality of life. Descriptive statistics were performed by nonparametric Mann-Whitney <i>U</i> and <i>χ</i> <sup>2</sup> tests for continuous and categorical variables, respectively.</p><p><strong>Results: </strong>Sixty patients were identified in the ERAS cohort versus 70 in the traditional pain control cohort. There was a statistically significant difference in average postoperative morphine equivalents received (17.0 vs. 39.9, <i>p</i> < 0.01) and average postoperative nursing pain score (2.4 vs. 3.6, <i>p</i> < 0.01). Fifty-three percent (32/60) of patients in the ERAS cohort received an opioid prescription for home compared with 80% (56/70) in the traditional cohort (<i>p</i> < 0.01). There was no significant quality-of-life difference between the groups. No adverse patient events resulted from the block.</p><p><strong>Conclusions: </strong>An ERAS pathway including a preoperative ESP block and multimodal analgesia decreased morphine equivalents received and nursing pain scores. Future randomized prospective studies with the ERAS protocol can be considered.</p>","PeriodicalId":39147,"journal":{"name":"Current Urology","volume":"19 5","pages":"343-346"},"PeriodicalIF":1.3000,"publicationDate":"2025-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398380/pdf/","citationCount":"0","resultStr":"{\"title\":\"Reducing pain and opioid use: Implementation of an enhanced recovery pathway for percutaneous nephrolithotomy with an erector spinae plane block.\",\"authors\":\"Aaron Saxton, David Song, Christopher Wanderling, Austin Lee, Timothy Campbell, Stephen Hassig, Yeon Joo Lee-Saxton, Sarah Jaffe, Kaitlyn Mitchell, Shlomi Tapiero, Rajat Jain, Scott O Quarrier\",\"doi\":\"10.1097/CU9.0000000000000283\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>There is no standard analgesic pathway after percutaneous nephrolithotomy. At our institution, an Enhanced Recovery After Surgery (ERAS) pathway was instated that included a preoperative erector spinae plane (ESP) block to improve pain control and minimize opioid usage in the postoperative setting.</p><p><strong>Materials and methods: </strong>At our institution, an ERAS pathway was created for patients undergoing percutaneous nephrolithotomy. This pathway involved a preoperative ESP block and the replacement of opioids with multimodal analgesia. Patient charts were retrospectively reviewed and placed into 2 cohorts: one cohort participated in the ERAS pathway, whereas the other received traditional pain control. The primary outcome evaluated was postoperative morphine equivalents received. Secondary outcomes included nursing pain scores, opioid prescriptions for home, and quality of life. Descriptive statistics were performed by nonparametric Mann-Whitney <i>U</i> and <i>χ</i> <sup>2</sup> tests for continuous and categorical variables, respectively.</p><p><strong>Results: </strong>Sixty patients were identified in the ERAS cohort versus 70 in the traditional pain control cohort. There was a statistically significant difference in average postoperative morphine equivalents received (17.0 vs. 39.9, <i>p</i> < 0.01) and average postoperative nursing pain score (2.4 vs. 3.6, <i>p</i> < 0.01). Fifty-three percent (32/60) of patients in the ERAS cohort received an opioid prescription for home compared with 80% (56/70) in the traditional cohort (<i>p</i> < 0.01). There was no significant quality-of-life difference between the groups. No adverse patient events resulted from the block.</p><p><strong>Conclusions: </strong>An ERAS pathway including a preoperative ESP block and multimodal analgesia decreased morphine equivalents received and nursing pain scores. Future randomized prospective studies with the ERAS protocol can be considered.</p>\",\"PeriodicalId\":39147,\"journal\":{\"name\":\"Current Urology\",\"volume\":\"19 5\",\"pages\":\"343-346\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2025-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12398380/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Current Urology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1097/CU9.0000000000000283\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2025/3/28 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Urology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CU9.0000000000000283","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/28 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Reducing pain and opioid use: Implementation of an enhanced recovery pathway for percutaneous nephrolithotomy with an erector spinae plane block.
Background: There is no standard analgesic pathway after percutaneous nephrolithotomy. At our institution, an Enhanced Recovery After Surgery (ERAS) pathway was instated that included a preoperative erector spinae plane (ESP) block to improve pain control and minimize opioid usage in the postoperative setting.
Materials and methods: At our institution, an ERAS pathway was created for patients undergoing percutaneous nephrolithotomy. This pathway involved a preoperative ESP block and the replacement of opioids with multimodal analgesia. Patient charts were retrospectively reviewed and placed into 2 cohorts: one cohort participated in the ERAS pathway, whereas the other received traditional pain control. The primary outcome evaluated was postoperative morphine equivalents received. Secondary outcomes included nursing pain scores, opioid prescriptions for home, and quality of life. Descriptive statistics were performed by nonparametric Mann-Whitney U and χ2 tests for continuous and categorical variables, respectively.
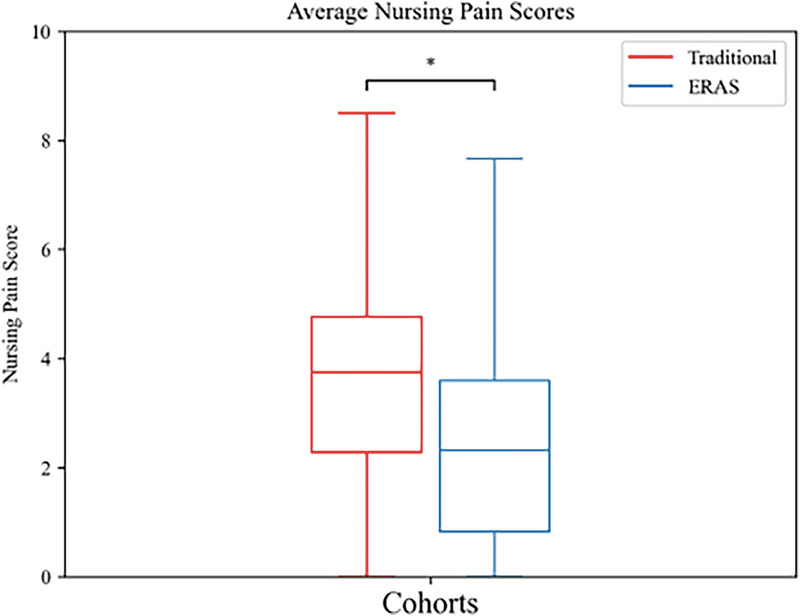
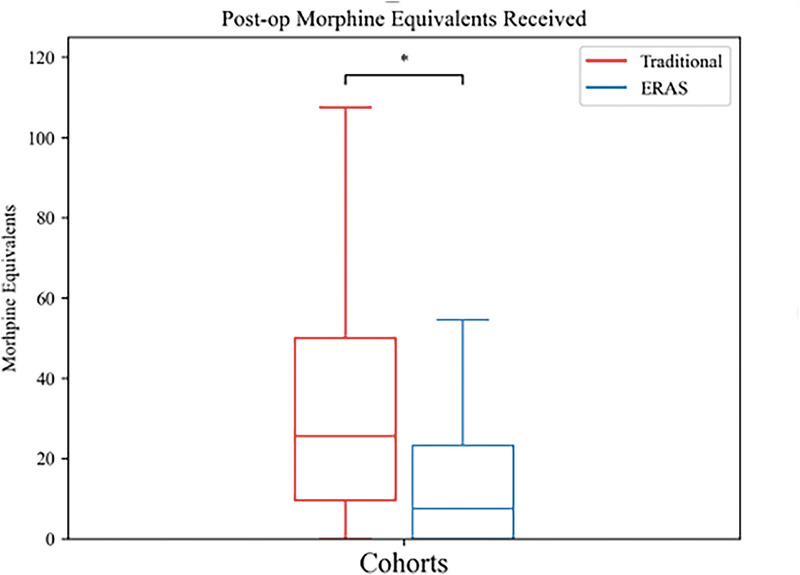
Results: Sixty patients were identified in the ERAS cohort versus 70 in the traditional pain control cohort. There was a statistically significant difference in average postoperative morphine equivalents received (17.0 vs. 39.9, p < 0.01) and average postoperative nursing pain score (2.4 vs. 3.6, p < 0.01). Fifty-three percent (32/60) of patients in the ERAS cohort received an opioid prescription for home compared with 80% (56/70) in the traditional cohort (p < 0.01). There was no significant quality-of-life difference between the groups. No adverse patient events resulted from the block.
Conclusions: An ERAS pathway including a preoperative ESP block and multimodal analgesia decreased morphine equivalents received and nursing pain scores. Future randomized prospective studies with the ERAS protocol can be considered.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


