George K Annan, Walter Agyeman, Samuel B Acheampong, Abigail Mills-Annoh, Albert Asare Adu
{"title":"肾梗死中一过性肾动脉狭窄1例报告。","authors":"George K Annan, Walter Agyeman, Samuel B Acheampong, Abigail Mills-Annoh, Albert Asare Adu","doi":"10.12659/AJCR.949596","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Renal infarction is a rare condition resulting from interruption of renal arterial blood flow. Its nonspecific presentation often mimics more common diagnoses such as nephrolithiasis, pyelonephritis, or musculoskeletal pain, contributing to delayed or missed diagnosis. Early identification is essential to prevent irreversible renal damage and optimize patient outcomes. Imaging plays a critical role in both the initial diagnosis and in determining the underlying etiology, which may include thromboembolism, in-situ thrombosis, vascular injury, or hypercoagulable states. CASE REPORT We describe a case of a 63-year-old woman with a history of coronary artery disease, diabetes mellitus, hormone replacement therapy, and a 42 pack-year smoking history, who presented with sudden-onset, severe left-flank pain. Initial laboratory results were nonspecific, with mild proteinuria and microscopic hematuria. Computed tomography (CT) angiography demonstrated severe stenosis of the superior left renal artery and extensive left renal infarction. A diagnosis of atherosclerotic renal infarction was made. She was treated with intravenous heparin, transitioned to dual antiplatelet therapy and high-intensity statin, and discharged with a 30-day cardiac event monitor. No arrhythmia was detected, and her thrombophilia workup was negative. Follow-up CT angiography 1 month later revealed complete resolution of the renal artery stenosis, with no residual narrowing or plaque. The transient nature of the vascular finding, along with the lack of structural atherosclerosis, prompted diagnostic reassessment, favoring an embolic mechanism possibly related to multiple modifiable prothrombotic clinical risk factors and unrecognized embolic sources. CONCLUSIONS This case illustrates the importance of follow-up imaging and clinical reassessment in differentiating embolic from atherosclerotic causes of renal infarction.</p>","PeriodicalId":39064,"journal":{"name":"American Journal of Case Reports","volume":"26 ","pages":"e949596"},"PeriodicalIF":0.7000,"publicationDate":"2025-08-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406750/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transient Renal Artery Stenosis in Renal Infarction: A Case Report.\",\"authors\":\"George K Annan, Walter Agyeman, Samuel B Acheampong, Abigail Mills-Annoh, Albert Asare Adu\",\"doi\":\"10.12659/AJCR.949596\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BACKGROUND Renal infarction is a rare condition resulting from interruption of renal arterial blood flow. Its nonspecific presentation often mimics more common diagnoses such as nephrolithiasis, pyelonephritis, or musculoskeletal pain, contributing to delayed or missed diagnosis. Early identification is essential to prevent irreversible renal damage and optimize patient outcomes. Imaging plays a critical role in both the initial diagnosis and in determining the underlying etiology, which may include thromboembolism, in-situ thrombosis, vascular injury, or hypercoagulable states. CASE REPORT We describe a case of a 63-year-old woman with a history of coronary artery disease, diabetes mellitus, hormone replacement therapy, and a 42 pack-year smoking history, who presented with sudden-onset, severe left-flank pain. Initial laboratory results were nonspecific, with mild proteinuria and microscopic hematuria. Computed tomography (CT) angiography demonstrated severe stenosis of the superior left renal artery and extensive left renal infarction. A diagnosis of atherosclerotic renal infarction was made. She was treated with intravenous heparin, transitioned to dual antiplatelet therapy and high-intensity statin, and discharged with a 30-day cardiac event monitor. No arrhythmia was detected, and her thrombophilia workup was negative. Follow-up CT angiography 1 month later revealed complete resolution of the renal artery stenosis, with no residual narrowing or plaque. The transient nature of the vascular finding, along with the lack of structural atherosclerosis, prompted diagnostic reassessment, favoring an embolic mechanism possibly related to multiple modifiable prothrombotic clinical risk factors and unrecognized embolic sources. CONCLUSIONS This case illustrates the importance of follow-up imaging and clinical reassessment in differentiating embolic from atherosclerotic causes of renal infarction.</p>\",\"PeriodicalId\":39064,\"journal\":{\"name\":\"American Journal of Case Reports\",\"volume\":\"26 \",\"pages\":\"e949596\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-08-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12406750/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12659/AJCR.949596\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.949596","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Transient Renal Artery Stenosis in Renal Infarction: A Case Report.
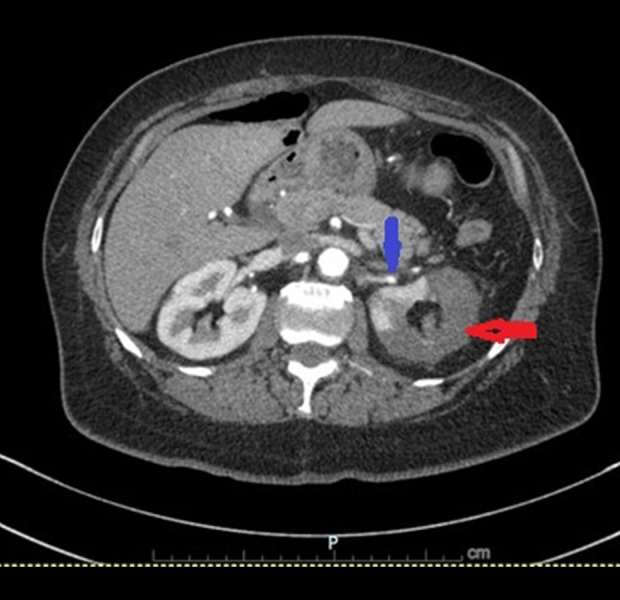
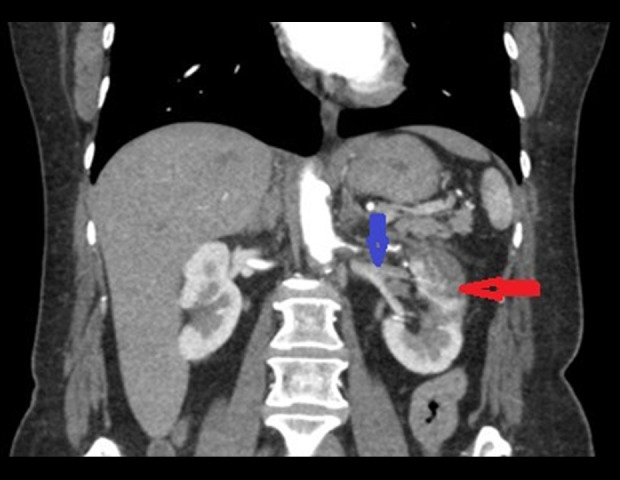
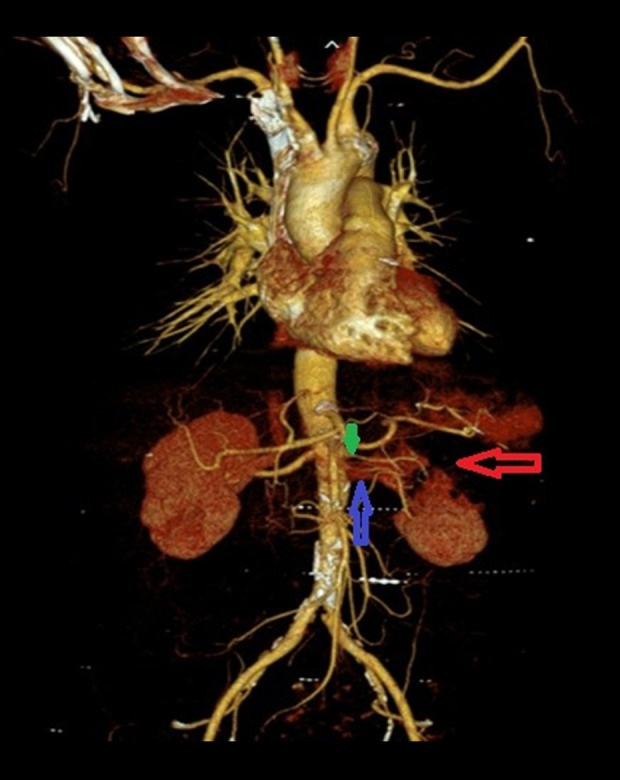
BACKGROUND Renal infarction is a rare condition resulting from interruption of renal arterial blood flow. Its nonspecific presentation often mimics more common diagnoses such as nephrolithiasis, pyelonephritis, or musculoskeletal pain, contributing to delayed or missed diagnosis. Early identification is essential to prevent irreversible renal damage and optimize patient outcomes. Imaging plays a critical role in both the initial diagnosis and in determining the underlying etiology, which may include thromboembolism, in-situ thrombosis, vascular injury, or hypercoagulable states. CASE REPORT We describe a case of a 63-year-old woman with a history of coronary artery disease, diabetes mellitus, hormone replacement therapy, and a 42 pack-year smoking history, who presented with sudden-onset, severe left-flank pain. Initial laboratory results were nonspecific, with mild proteinuria and microscopic hematuria. Computed tomography (CT) angiography demonstrated severe stenosis of the superior left renal artery and extensive left renal infarction. A diagnosis of atherosclerotic renal infarction was made. She was treated with intravenous heparin, transitioned to dual antiplatelet therapy and high-intensity statin, and discharged with a 30-day cardiac event monitor. No arrhythmia was detected, and her thrombophilia workup was negative. Follow-up CT angiography 1 month later revealed complete resolution of the renal artery stenosis, with no residual narrowing or plaque. The transient nature of the vascular finding, along with the lack of structural atherosclerosis, prompted diagnostic reassessment, favoring an embolic mechanism possibly related to multiple modifiable prothrombotic clinical risk factors and unrecognized embolic sources. CONCLUSIONS This case illustrates the importance of follow-up imaging and clinical reassessment in differentiating embolic from atherosclerotic causes of renal infarction.
期刊介绍:
American Journal of Case Reports is an international, peer-reviewed scientific journal that publishes single and series case reports in all medical fields. American Journal of Case Reports is issued on a continuous basis as a primary electronic journal. Print copies of a single article or a set of articles can be ordered on demand.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


