Cassandra L Stegall, Brendon Carnell, Jamie M Golden, Rupa Kapoor, John H Fanton, Paul C Mullan, Alexandra P Leader
{"title":"多学科致命手段安全咨询设计和实施:培训和识别障碍在儿童医院。","authors":"Cassandra L Stegall, Brendon Carnell, Jamie M Golden, Rupa Kapoor, John H Fanton, Paul C Mullan, Alexandra P Leader","doi":"10.1186/s40621-025-00599-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Access to lethal means contributes significantly to suicide completion. Lethal means safety counseling (LMSC) is an injury prevention strategy to limit access to firearms, medications, and other means of injury. Not previously evaluated in the trauma setting, this study aims to design and implement a standardized LMSC protocol for pediatric patient discharge education in emergency (ED), trauma, and inpatient psychiatry settings.</p><p><strong>Methods: </strong>A single-center quality improvement study at an academic pediatric urban tertiary Level-one trauma center was performed from July 2023 to February 2024. Protocol was implemented for pediatric patients discharged from three departments: ED, surgery trauma service, and psychiatry. Interventions included electronic medical record (EMR) based LMSC screening questions, training with Counseling on Access to Lethal Means (CALM) module, a de novo educational training video, and providing families free cable gun locks and medicine lock boxes. Healthcare collaborators completed pre- and post-training surveys. Data was recorded in Redcap and analyzed as descriptive and parametric data. Primary outcome was incorporation of LMSC and intervention into social worker's workflow. Secondary outcomes included project barriers and outcomes, familial impression of counseling, and healthcare provider impression of intervention.</p><p><strong>Results: </strong>Out of forty-eight persons, 29 providers completed the pre-training survey and 17 completed the post-training survey. Results indicated increased discussions with caregivers about safe medicine storage comparing averages of pre and post-test results (mean difference 0.44, 95% CI 0.05-0.83, p = 0.029), but no differences in discussions about safe firearm storage (mean difference 0.50, 95% CI - 0.05-1.05, p = 0.07) or knives (mean difference 0.56, 95% CI 0.05-1.18 p = 0.07). Provider behavior changes occurred with increased clinical frequency of cable gun lock distribution.</p><p><strong>Conclusions: </strong>This study describes implementing a standardized LMSC protocol in three pediatric hospital departments with self-reported provider improvements in LMSC. Barriers identified to protocol implementation are an opportunity to improve future preventative patient care.</p>","PeriodicalId":37379,"journal":{"name":"Injury Epidemiology","volume":"12 1","pages":"52"},"PeriodicalIF":2.2000,"publicationDate":"2025-08-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12395793/pdf/","citationCount":"0","resultStr":"{\"title\":\"Multidisciplinary lethal means safety counseling design and implementation: training and identifying barriers in a children's hospital.\",\"authors\":\"Cassandra L Stegall, Brendon Carnell, Jamie M Golden, Rupa Kapoor, John H Fanton, Paul C Mullan, Alexandra P Leader\",\"doi\":\"10.1186/s40621-025-00599-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Access to lethal means contributes significantly to suicide completion. Lethal means safety counseling (LMSC) is an injury prevention strategy to limit access to firearms, medications, and other means of injury. Not previously evaluated in the trauma setting, this study aims to design and implement a standardized LMSC protocol for pediatric patient discharge education in emergency (ED), trauma, and inpatient psychiatry settings.</p><p><strong>Methods: </strong>A single-center quality improvement study at an academic pediatric urban tertiary Level-one trauma center was performed from July 2023 to February 2024. Protocol was implemented for pediatric patients discharged from three departments: ED, surgery trauma service, and psychiatry. Interventions included electronic medical record (EMR) based LMSC screening questions, training with Counseling on Access to Lethal Means (CALM) module, a de novo educational training video, and providing families free cable gun locks and medicine lock boxes. Healthcare collaborators completed pre- and post-training surveys. Data was recorded in Redcap and analyzed as descriptive and parametric data. Primary outcome was incorporation of LMSC and intervention into social worker's workflow. Secondary outcomes included project barriers and outcomes, familial impression of counseling, and healthcare provider impression of intervention.</p><p><strong>Results: </strong>Out of forty-eight persons, 29 providers completed the pre-training survey and 17 completed the post-training survey. Results indicated increased discussions with caregivers about safe medicine storage comparing averages of pre and post-test results (mean difference 0.44, 95% CI 0.05-0.83, p = 0.029), but no differences in discussions about safe firearm storage (mean difference 0.50, 95% CI - 0.05-1.05, p = 0.07) or knives (mean difference 0.56, 95% CI 0.05-1.18 p = 0.07). Provider behavior changes occurred with increased clinical frequency of cable gun lock distribution.</p><p><strong>Conclusions: </strong>This study describes implementing a standardized LMSC protocol in three pediatric hospital departments with self-reported provider improvements in LMSC. Barriers identified to protocol implementation are an opportunity to improve future preventative patient care.</p>\",\"PeriodicalId\":37379,\"journal\":{\"name\":\"Injury Epidemiology\",\"volume\":\"12 1\",\"pages\":\"52\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2025-08-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12395793/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Injury Epidemiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s40621-025-00599-5\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Injury Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40621-025-00599-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
摘要
背景:获得致命手段对自杀完成有重大贡献。致命手段安全咨询(LMSC)是一种伤害预防策略,以限制获得枪支,药物和其他伤害手段。本研究旨在为急诊(ED)、创伤和住院精神科儿科患者的出院教育设计和实施标准化的LMSC协议,此前未在创伤环境中进行评估。方法:于2023年7月至2024年2月在某学术性儿科城市三级创伤中心进行单中心质量改善研究。在三个科室:急诊科、外科创伤科和精神科出院的儿科患者中实施了协议。干预措施包括基于电子医疗记录(EMR)的LMSC筛查问题,使用获取致命手段咨询(CALM)模块进行培训,一个全新的教育培训视频,以及向家庭提供免费的电缆枪锁和药箱。医疗保健合作者完成了培训前和培训后的调查。数据记录在Redcap中,并作为描述性和参数性数据进行分析。主要结果是将LMSC和干预纳入社会工作者的工作流程。次要结局包括项目障碍和结果、家庭对咨询的印象和医疗保健提供者对干预的印象。结果:48人中,29人完成了培训前调查,17人完成了培训后调查。结果显示,与检测前后的平均结果相比,与护理人员讨论安全药物储存的次数增加(平均差异0.44,95% CI 0.05-0.83, p = 0.029),但讨论安全枪支储存的次数无差异(平均差异0.50,95% CI - 0.05-1.05, p = 0.07)或刀具(平均差异0.56,95% CI 0.05-1.18 p = 0.07)。提供者的行为随着缆枪锁定分布频率的增加而发生变化。结论:本研究描述了在三个儿科医院部门实施标准化LMSC协议,并自我报告提供者在LMSC方面的改进。确定协议实施的障碍是改善未来预防性患者护理的机会。
Multidisciplinary lethal means safety counseling design and implementation: training and identifying barriers in a children's hospital.
Background: Access to lethal means contributes significantly to suicide completion. Lethal means safety counseling (LMSC) is an injury prevention strategy to limit access to firearms, medications, and other means of injury. Not previously evaluated in the trauma setting, this study aims to design and implement a standardized LMSC protocol for pediatric patient discharge education in emergency (ED), trauma, and inpatient psychiatry settings.
Methods: A single-center quality improvement study at an academic pediatric urban tertiary Level-one trauma center was performed from July 2023 to February 2024. Protocol was implemented for pediatric patients discharged from three departments: ED, surgery trauma service, and psychiatry. Interventions included electronic medical record (EMR) based LMSC screening questions, training with Counseling on Access to Lethal Means (CALM) module, a de novo educational training video, and providing families free cable gun locks and medicine lock boxes. Healthcare collaborators completed pre- and post-training surveys. Data was recorded in Redcap and analyzed as descriptive and parametric data. Primary outcome was incorporation of LMSC and intervention into social worker's workflow. Secondary outcomes included project barriers and outcomes, familial impression of counseling, and healthcare provider impression of intervention.
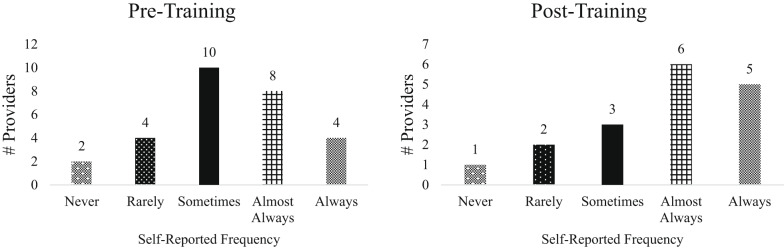
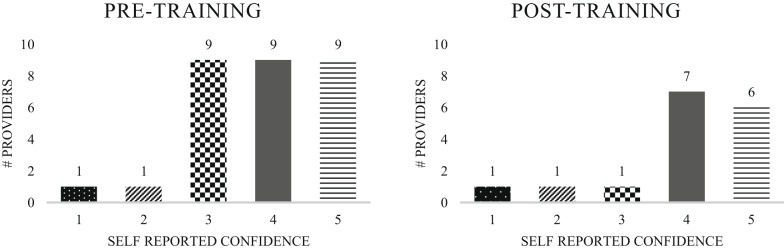
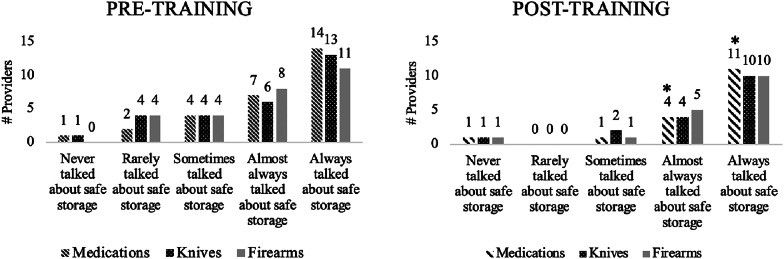
Results: Out of forty-eight persons, 29 providers completed the pre-training survey and 17 completed the post-training survey. Results indicated increased discussions with caregivers about safe medicine storage comparing averages of pre and post-test results (mean difference 0.44, 95% CI 0.05-0.83, p = 0.029), but no differences in discussions about safe firearm storage (mean difference 0.50, 95% CI - 0.05-1.05, p = 0.07) or knives (mean difference 0.56, 95% CI 0.05-1.18 p = 0.07). Provider behavior changes occurred with increased clinical frequency of cable gun lock distribution.
Conclusions: This study describes implementing a standardized LMSC protocol in three pediatric hospital departments with self-reported provider improvements in LMSC. Barriers identified to protocol implementation are an opportunity to improve future preventative patient care.
期刊介绍:
Injury Epidemiology is dedicated to advancing the scientific foundation for injury prevention and control through timely publication and dissemination of peer-reviewed research. Injury Epidemiology aims to be the premier venue for communicating epidemiologic studies of unintentional and intentional injuries, including, but not limited to, morbidity and mortality from motor vehicle crashes, drug overdose/poisoning, falls, drowning, fires/burns, iatrogenic injury, suicide, homicide, assaults, and abuse. We welcome investigations designed to understand the magnitude, distribution, determinants, causes, prevention, diagnosis, treatment, prognosis, and outcomes of injuries in specific population groups, geographic regions, and environmental settings (e.g., home, workplace, transport, recreation, sports, and urban/rural). Injury Epidemiology has a special focus on studies generating objective and practical knowledge that can be translated into interventions to reduce injury morbidity and mortality on a population level. Priority consideration will be given to manuscripts that feature contemporary theories and concepts, innovative methods, and novel techniques as applied to injury surveillance, risk assessment, development and implementation of effective interventions, and program and policy evaluation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


