Selina Marie Kronthaler, Tatjana Tissen-Diabaté, Maria Margarete Karsten, Jens-Uwe Blohmer, Klaus Michael Beier, Laura Hatzler
{"title":"评估精神和慢性健康状况作为性功能障碍妇女保健需求和数字创新的决定因素:德国基于人口的横断面调查研究","authors":"Selina Marie Kronthaler, Tatjana Tissen-Diabaté, Maria Margarete Karsten, Jens-Uwe Blohmer, Klaus Michael Beier, Laura Hatzler","doi":"10.2196/71301","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A chronic health condition (CHC) is a recognized risk factor for experiencing problems in sexual function (PSF). According to the International Classification of Diseases, 11th Revision (ICD-11), the development of severe symptoms of sexual distress is the defining criterion for clinically relevant sexual dysfunction. Data on the contribution of specific CHCs to clinically relevant sexual dysfunction symptoms and related health care needs are limited, hindering targeted interventions.</p><p><strong>Objective: </strong>This study examines the prevalence of PSF, sexual dysfunction, and sexual distress; assesses associations with CHC status; evaluates sexual dysfunction diagnoses; and explores health care preferences.</p><p><strong>Methods: </strong>Data collection in this cross-sectional population-based survey study was based on a questionnaire developed with patient and public involvement and administered by YouGov to a representative sample of adults in Germany. Analyses included 1970 women with and without CHCs and different CHC subgroups (mental health-related, gynecological, cardiovascular and metabolic, infectious and inflammatory, cancer, pain-related, and neurological). The outcomes measured were PSF, clinically relevant sexual dysfunction symptoms, sexual distress (Female Sexual Distress Scale-Desire/Arousal/Orgasm [FSDS-DAO]), and self-reported sexual dysfunction diagnoses. Multivariable regression and network analysis explored associations among CHC subgroups, PSF, sexual dysfunction, and FSDS-DAO scores.</p><p><strong>Results: </strong>Among 1970 cisgender women (mean age 49.6, SD 16.0 years), 1186 (60.2%) reported CHCs. The 6-month PSF prevalence was 75.2% (820/1090) in women with CHCs and 62.5% (399/638) in women without CHCs. Clinically relevant sexual dysfunction symptoms were less prevalent (CHC: 202/1046, 19.3% vs no CHC: 68/601, 11.3%). Multivariable regression models showed an association between sexual dysfunction and CHCs (odds ratio [OR] 2.56, 95% CI 1.90-3.49), which was the strongest for women with mental health-related CHCs (OR 2.31, 95% CI 1.70-3.13) and cancer CHCs (OR 2.00, 95% CI 1.45-2.78). Being in a relationship was a protective factor for clinically relevant distress among women with CHCs. Network analysis showed positive associations of PSF with gynecological and mental health-related CHCs and of sexual dysfunction with mental health-related, gynecological, and cancer CHCs. Women with sexual dysfunction symptoms reported low rates of sexual dysfunction diagnosis (CHC: 39/200, 19.4% vs no CHC: 6/55, 10.7%) and treatment (CHC: 16/146, 11.0% vs no CHC: 3/40, 7.0%). Gynecologists were the preferred health care providers for sexual dysfunction. The most commonly reported unmet need was a lack of information. Digital solutions, such as apps and websites with exercises, were desired as health care innovations.</p><p><strong>Conclusions: </strong>The burden of CHCs on women's sexual health extends beyond functional sexual impairment, with high rates of clinically relevant sexual distress. Cancer and mental health conditions are the strongest predictors of sexual dysfunction. Despite the high prevalence of sexual dysfunction in women with CHCs, access to diagnosis and treatment is limited. Digital offerings could help address these unmet needs.</p>","PeriodicalId":36208,"journal":{"name":"Journal of Participatory Medicine","volume":"17 ","pages":"e71301"},"PeriodicalIF":0.0000,"publicationDate":"2025-08-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386550/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessment of Mental and Chronic Health Conditions as Determinants of Health Care Needs and Digital Innovations for Women With Sexual Dysfunction: Cross-Sectional Population-Based Survey Study in Germany.\",\"authors\":\"Selina Marie Kronthaler, Tatjana Tissen-Diabaté, Maria Margarete Karsten, Jens-Uwe Blohmer, Klaus Michael Beier, Laura Hatzler\",\"doi\":\"10.2196/71301\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>A chronic health condition (CHC) is a recognized risk factor for experiencing problems in sexual function (PSF). According to the International Classification of Diseases, 11th Revision (ICD-11), the development of severe symptoms of sexual distress is the defining criterion for clinically relevant sexual dysfunction. Data on the contribution of specific CHCs to clinically relevant sexual dysfunction symptoms and related health care needs are limited, hindering targeted interventions.</p><p><strong>Objective: </strong>This study examines the prevalence of PSF, sexual dysfunction, and sexual distress; assesses associations with CHC status; evaluates sexual dysfunction diagnoses; and explores health care preferences.</p><p><strong>Methods: </strong>Data collection in this cross-sectional population-based survey study was based on a questionnaire developed with patient and public involvement and administered by YouGov to a representative sample of adults in Germany. Analyses included 1970 women with and without CHCs and different CHC subgroups (mental health-related, gynecological, cardiovascular and metabolic, infectious and inflammatory, cancer, pain-related, and neurological). The outcomes measured were PSF, clinically relevant sexual dysfunction symptoms, sexual distress (Female Sexual Distress Scale-Desire/Arousal/Orgasm [FSDS-DAO]), and self-reported sexual dysfunction diagnoses. Multivariable regression and network analysis explored associations among CHC subgroups, PSF, sexual dysfunction, and FSDS-DAO scores.</p><p><strong>Results: </strong>Among 1970 cisgender women (mean age 49.6, SD 16.0 years), 1186 (60.2%) reported CHCs. The 6-month PSF prevalence was 75.2% (820/1090) in women with CHCs and 62.5% (399/638) in women without CHCs. Clinically relevant sexual dysfunction symptoms were less prevalent (CHC: 202/1046, 19.3% vs no CHC: 68/601, 11.3%). Multivariable regression models showed an association between sexual dysfunction and CHCs (odds ratio [OR] 2.56, 95% CI 1.90-3.49), which was the strongest for women with mental health-related CHCs (OR 2.31, 95% CI 1.70-3.13) and cancer CHCs (OR 2.00, 95% CI 1.45-2.78). Being in a relationship was a protective factor for clinically relevant distress among women with CHCs. Network analysis showed positive associations of PSF with gynecological and mental health-related CHCs and of sexual dysfunction with mental health-related, gynecological, and cancer CHCs. Women with sexual dysfunction symptoms reported low rates of sexual dysfunction diagnosis (CHC: 39/200, 19.4% vs no CHC: 6/55, 10.7%) and treatment (CHC: 16/146, 11.0% vs no CHC: 3/40, 7.0%). Gynecologists were the preferred health care providers for sexual dysfunction. The most commonly reported unmet need was a lack of information. Digital solutions, such as apps and websites with exercises, were desired as health care innovations.</p><p><strong>Conclusions: </strong>The burden of CHCs on women's sexual health extends beyond functional sexual impairment, with high rates of clinically relevant sexual distress. Cancer and mental health conditions are the strongest predictors of sexual dysfunction. Despite the high prevalence of sexual dysfunction in women with CHCs, access to diagnosis and treatment is limited. Digital offerings could help address these unmet needs.</p>\",\"PeriodicalId\":36208,\"journal\":{\"name\":\"Journal of Participatory Medicine\",\"volume\":\"17 \",\"pages\":\"e71301\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2025-08-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12386550/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Participatory Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.2196/71301\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Participatory Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/71301","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:慢性健康状况(CHC)是经历性功能问题(PSF)的公认危险因素。根据《国际疾病分类》第11版(ICD-11),出现严重的性困扰症状是临床上相关性功能障碍的定义标准。关于特定CHCs对临床相关性功能障碍症状和相关卫生保健需求的贡献的数据有限,妨碍了有针对性的干预。目的:本研究探讨了PSF、性功能障碍和性困扰的患病率;评估与CHC状况的关联;评估性功能障碍诊断;并探讨了医疗保健的偏好。方法:在这项以人口为基础的横断面调查研究中,数据收集基于一份由YouGov对德国成年人的代表性样本进行的问卷调查,该问卷由患者和公众参与。分析包括1970名患有和不患有CHC的妇女以及不同的CHC亚组(精神健康相关、妇科、心血管和代谢、感染和炎症、癌症、疼痛相关和神经系统)。测量结果包括PSF、临床相关性功能障碍症状、性困扰(女性性困扰量表-欲望/觉醒/性高潮[FSDS-DAO])和自我报告的性功能障碍诊断。多变量回归和网络分析探讨了CHC亚组、PSF、性功能障碍和FSDS-DAO评分之间的关系。结果:1970例顺性别女性(平均年龄49.6岁,SD 16.0岁)中,1186例(60.2%)报告CHCs。CHCs患者6个月PSF患病率为75.2%(820/1090),非CHCs患者为62.5%(399/638)。临床相关性功能障碍症状较少见(CHC: 202/1046, 19.3% vs无CHC: 68/601, 11.3%)。多变量回归模型显示性功能障碍与CHCs之间存在关联(比值比[OR] 2.56, 95% CI 1.90-3.49),其中与精神健康相关的CHCs (OR 2.31, 95% CI 1.70-3.13)和癌症CHCs (OR 2.00, 95% CI 1.45-2.78)的女性相关性最强。在患有CHCs的女性中,处于恋爱关系是临床相关痛苦的保护因素。网络分析显示PSF与妇科和精神健康相关的CHCs呈正相关,性功能障碍与精神健康相关、妇科和癌症相关的CHCs呈正相关。有性功能障碍症状的女性性功能障碍诊断率低(CHC: 39/200, 19.4%,无CHC: 6/55, 10.7%),治疗率低(CHC: 16/146, 11.0%,无CHC: 3/40, 7.0%)。妇科医生是性功能障碍患者的首选医疗保健提供者。最常见的未满足需求是缺乏信息。数字解决方案,如锻炼应用程序和网站,被视为医疗保健创新。结论:CHCs对女性性健康的负担超出了功能性性功能障碍的范畴,其临床相关性困扰的发生率很高。癌症和精神健康状况是性功能障碍的最强预测因子。尽管CHCs女性性功能障碍的患病率很高,但诊断和治疗的机会有限。数字产品可以帮助解决这些未满足的需求。
Assessment of Mental and Chronic Health Conditions as Determinants of Health Care Needs and Digital Innovations for Women With Sexual Dysfunction: Cross-Sectional Population-Based Survey Study in Germany.
Background: A chronic health condition (CHC) is a recognized risk factor for experiencing problems in sexual function (PSF). According to the International Classification of Diseases, 11th Revision (ICD-11), the development of severe symptoms of sexual distress is the defining criterion for clinically relevant sexual dysfunction. Data on the contribution of specific CHCs to clinically relevant sexual dysfunction symptoms and related health care needs are limited, hindering targeted interventions.
Objective: This study examines the prevalence of PSF, sexual dysfunction, and sexual distress; assesses associations with CHC status; evaluates sexual dysfunction diagnoses; and explores health care preferences.
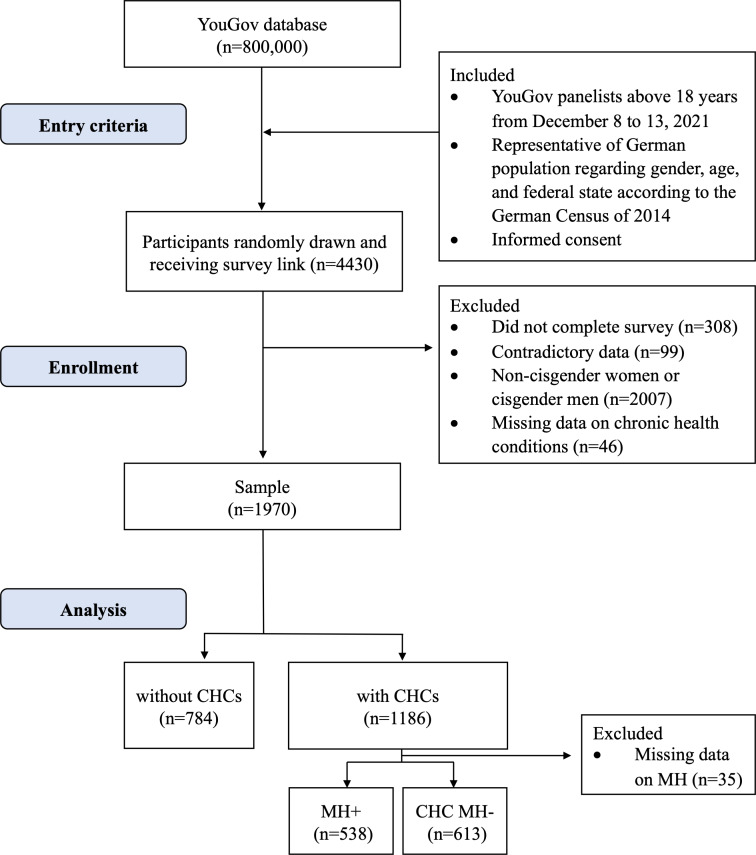
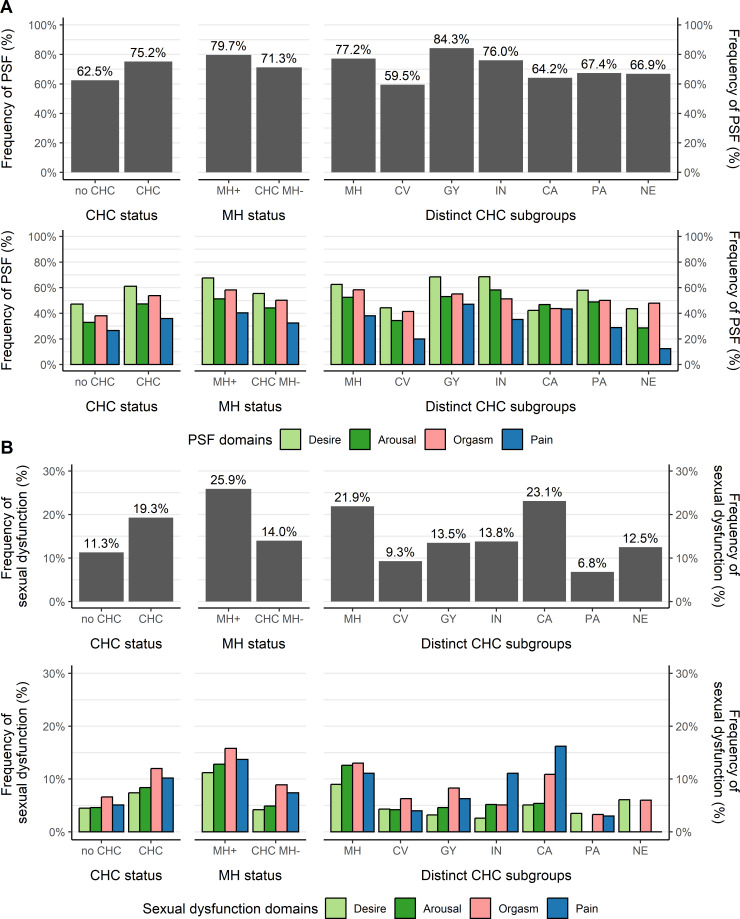
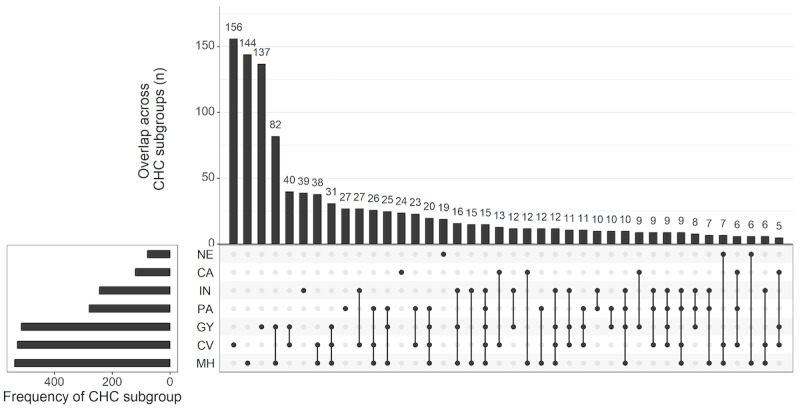
Methods: Data collection in this cross-sectional population-based survey study was based on a questionnaire developed with patient and public involvement and administered by YouGov to a representative sample of adults in Germany. Analyses included 1970 women with and without CHCs and different CHC subgroups (mental health-related, gynecological, cardiovascular and metabolic, infectious and inflammatory, cancer, pain-related, and neurological). The outcomes measured were PSF, clinically relevant sexual dysfunction symptoms, sexual distress (Female Sexual Distress Scale-Desire/Arousal/Orgasm [FSDS-DAO]), and self-reported sexual dysfunction diagnoses. Multivariable regression and network analysis explored associations among CHC subgroups, PSF, sexual dysfunction, and FSDS-DAO scores.
Results: Among 1970 cisgender women (mean age 49.6, SD 16.0 years), 1186 (60.2%) reported CHCs. The 6-month PSF prevalence was 75.2% (820/1090) in women with CHCs and 62.5% (399/638) in women without CHCs. Clinically relevant sexual dysfunction symptoms were less prevalent (CHC: 202/1046, 19.3% vs no CHC: 68/601, 11.3%). Multivariable regression models showed an association between sexual dysfunction and CHCs (odds ratio [OR] 2.56, 95% CI 1.90-3.49), which was the strongest for women with mental health-related CHCs (OR 2.31, 95% CI 1.70-3.13) and cancer CHCs (OR 2.00, 95% CI 1.45-2.78). Being in a relationship was a protective factor for clinically relevant distress among women with CHCs. Network analysis showed positive associations of PSF with gynecological and mental health-related CHCs and of sexual dysfunction with mental health-related, gynecological, and cancer CHCs. Women with sexual dysfunction symptoms reported low rates of sexual dysfunction diagnosis (CHC: 39/200, 19.4% vs no CHC: 6/55, 10.7%) and treatment (CHC: 16/146, 11.0% vs no CHC: 3/40, 7.0%). Gynecologists were the preferred health care providers for sexual dysfunction. The most commonly reported unmet need was a lack of information. Digital solutions, such as apps and websites with exercises, were desired as health care innovations.
Conclusions: The burden of CHCs on women's sexual health extends beyond functional sexual impairment, with high rates of clinically relevant sexual distress. Cancer and mental health conditions are the strongest predictors of sexual dysfunction. Despite the high prevalence of sexual dysfunction in women with CHCs, access to diagnosis and treatment is limited. Digital offerings could help address these unmet needs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


