{"title":"系统性红斑狼疮发作伴明显心包积液时心脏填塞的处理:1例报告。","authors":"Adam D Walsh, Mitchell T Carroll","doi":"10.12659/AJCR.947859","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Pericarditis is a frequently encountered complication of systemic lupus erythematosus (SLE). However, cardiac tamponade resulting from massive pericardial effusion is a rare sequela. Risk factors for cardiac tamponade in SLE include female sex, reduced serum complement, and positive anti-nucleosome antibody at diagnosis. Management options for cardiac tamponade, such as pericardiocentesis and pericardial window, are tailored to the individual, and clear guidelines for when to proceed with invasive intervention are lacking. CASE REPORT We present a case of cardiac tamponade associated with an SLE exacerbation in a 38-year-old woman, associated with fever, dyspnea, and pleuritic chest pain. A chest radiograph demonstrated a large left pleural effusion obscuring a widened mediastinum suspicious for pericardial effusion. After a trial of medical therapy, the patient developed new atrial fibrillation, hypotension, and tachycardia, and proceeded to pericardiocentesis following which 1.6 liters of pericardial fluid was drained over the following 24 hours. Disease control was achieved with high-dose pulsed corticosteroids and cyclophosphamide and there was no recurrence of the effusion. CONCLUSIONS This appears to be one of the largest volumes of pericardial drainage described in the literature in the setting of SLE. Cardiac tamponade can occur at any stage of the disease course in SLE. Large pleural effusions can mimic symptoms of pericardial effusion and make diagnosis challenging. Definitive management can be achieved using a combination of invasive and medical therapy. Risk factors for the development of cardiac tamponade should be identified early in the course of an SLE exacerbation to ensure prompt treatment and avoid further complications.</p>","PeriodicalId":39064,"journal":{"name":"American Journal of Case Reports","volume":"26 ","pages":"e947859"},"PeriodicalIF":0.7000,"publicationDate":"2025-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392845/pdf/","citationCount":"0","resultStr":"{\"title\":\"Management of Cardiac Tamponade During Systemic Lupus Erythematosus Flare with Significant Pericardial Effusion: A Case Report.\",\"authors\":\"Adam D Walsh, Mitchell T Carroll\",\"doi\":\"10.12659/AJCR.947859\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BACKGROUND Pericarditis is a frequently encountered complication of systemic lupus erythematosus (SLE). However, cardiac tamponade resulting from massive pericardial effusion is a rare sequela. Risk factors for cardiac tamponade in SLE include female sex, reduced serum complement, and positive anti-nucleosome antibody at diagnosis. Management options for cardiac tamponade, such as pericardiocentesis and pericardial window, are tailored to the individual, and clear guidelines for when to proceed with invasive intervention are lacking. CASE REPORT We present a case of cardiac tamponade associated with an SLE exacerbation in a 38-year-old woman, associated with fever, dyspnea, and pleuritic chest pain. A chest radiograph demonstrated a large left pleural effusion obscuring a widened mediastinum suspicious for pericardial effusion. After a trial of medical therapy, the patient developed new atrial fibrillation, hypotension, and tachycardia, and proceeded to pericardiocentesis following which 1.6 liters of pericardial fluid was drained over the following 24 hours. Disease control was achieved with high-dose pulsed corticosteroids and cyclophosphamide and there was no recurrence of the effusion. CONCLUSIONS This appears to be one of the largest volumes of pericardial drainage described in the literature in the setting of SLE. Cardiac tamponade can occur at any stage of the disease course in SLE. Large pleural effusions can mimic symptoms of pericardial effusion and make diagnosis challenging. Definitive management can be achieved using a combination of invasive and medical therapy. Risk factors for the development of cardiac tamponade should be identified early in the course of an SLE exacerbation to ensure prompt treatment and avoid further complications.</p>\",\"PeriodicalId\":39064,\"journal\":{\"name\":\"American Journal of Case Reports\",\"volume\":\"26 \",\"pages\":\"e947859\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-08-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12392845/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12659/AJCR.947859\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.947859","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Management of Cardiac Tamponade During Systemic Lupus Erythematosus Flare with Significant Pericardial Effusion: A Case Report.
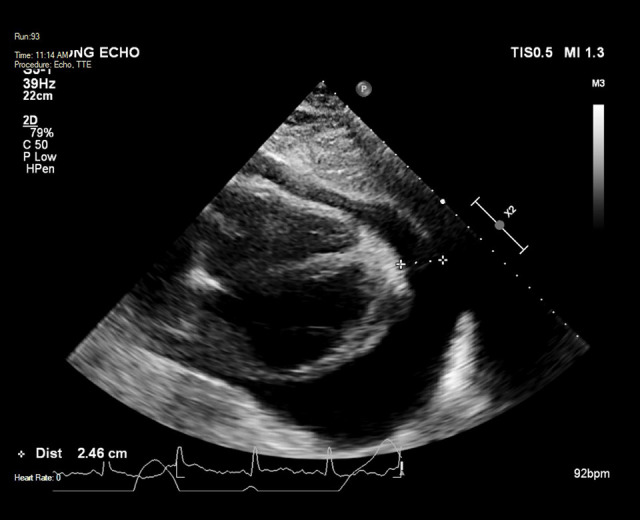
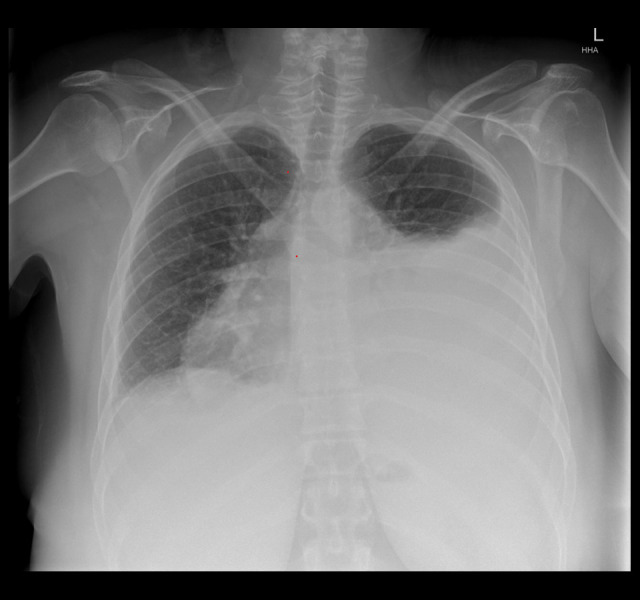
BACKGROUND Pericarditis is a frequently encountered complication of systemic lupus erythematosus (SLE). However, cardiac tamponade resulting from massive pericardial effusion is a rare sequela. Risk factors for cardiac tamponade in SLE include female sex, reduced serum complement, and positive anti-nucleosome antibody at diagnosis. Management options for cardiac tamponade, such as pericardiocentesis and pericardial window, are tailored to the individual, and clear guidelines for when to proceed with invasive intervention are lacking. CASE REPORT We present a case of cardiac tamponade associated with an SLE exacerbation in a 38-year-old woman, associated with fever, dyspnea, and pleuritic chest pain. A chest radiograph demonstrated a large left pleural effusion obscuring a widened mediastinum suspicious for pericardial effusion. After a trial of medical therapy, the patient developed new atrial fibrillation, hypotension, and tachycardia, and proceeded to pericardiocentesis following which 1.6 liters of pericardial fluid was drained over the following 24 hours. Disease control was achieved with high-dose pulsed corticosteroids and cyclophosphamide and there was no recurrence of the effusion. CONCLUSIONS This appears to be one of the largest volumes of pericardial drainage described in the literature in the setting of SLE. Cardiac tamponade can occur at any stage of the disease course in SLE. Large pleural effusions can mimic symptoms of pericardial effusion and make diagnosis challenging. Definitive management can be achieved using a combination of invasive and medical therapy. Risk factors for the development of cardiac tamponade should be identified early in the course of an SLE exacerbation to ensure prompt treatment and avoid further complications.
期刊介绍:
American Journal of Case Reports is an international, peer-reviewed scientific journal that publishes single and series case reports in all medical fields. American Journal of Case Reports is issued on a continuous basis as a primary electronic journal. Print copies of a single article or a set of articles can be ordered on demand.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


