{"title":"基于免疫检查点抑制剂接受全身治疗的肝癌患者急性静脉曲张出血的风险预测","authors":"Xu Zhang, Li-Meng Song, Yu-Piao Zheng, Bao-Xin Qian, Jing Liang, Feng-Mei Wang","doi":"10.4251/wjgo.v17.i8.108887","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute variceal bleeding (AVB) represents a life-threatening complication in hepatocellular carcinoma (HCC) patients undergoing systemic therapy, mainly including immune checkpoint inhibitors (ICIs) and antivascular drugs used alone or in combination. The pathogenesis of AVB in this population may involve tumor-related factors, treatment-induced effects, or progression of underlying portal hypertension. Identifying high-risk factors for AVB is crucial for the management of this patient population.</p><p><strong>Aim: </strong>To develop and validate a risk prediction model for AVB occurrence in cirrhotic HCC patients receiving ICI-based systemic therapy.</p><p><strong>Methods: </strong>This retrospective study analyzed 286 HCC patients (2021-2022) receiving ICIs (mono-/combination therapy), randomly split into training (<i>n</i> = 184) and validation (<i>n</i> = 102) cohorts. In the training cohort, bleeding <i>vs</i> non-bleeding groups were compared for general information, etiological data, laboratory indicators, tumor staging, systemic treatment drugs, variceal bleeding history, and endoscopic treatment history. Risk factors for AVB were identified and used to establish a logistic regression model for predicting bleeding, which was further validated in the validation cohort.</p><p><strong>Results: </strong>The bleeding group had significantly higher proportions of patients with platelet count ≥ 100 × 10<sup>9</sup>/L, alpha-fetoprotein ≥ 400 ng/mL, tumor diameter ≥ 5 cm, portal vein tumor thrombosis, ascites, bleeding history, prior endoscopic treatment, albumin-bilirubin grade level 2-3, fibrosis-4 index (FIB-4) ≥ 4.57, and prognostic nutritional index < 45 compared to the non-bleeding group. Multivariate analysis identified tumor diameter ≥ 5 cm, portal vein thrombosis, bleeding history, and elevated FIB-4 as independent risk factors for bleeding (<i>P</i> < 0.05). A predictive model based on these factors showed good discrimination, with area under the receiver operating characteristic curve values of 0.861 (training) and 0.816 (validation).</p><p><strong>Conclusion: </strong>A history of pre-ICI bleeding significantly increases recurrent bleeding risk, necessitating close monitoring. The FIB-4 fibrosis model, combined with tumor features, can also serve as a predictive factor for bleeding.</p>","PeriodicalId":23762,"journal":{"name":"World Journal of Gastrointestinal Oncology","volume":"17 8","pages":"108887"},"PeriodicalIF":2.5000,"publicationDate":"2025-08-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12362552/pdf/","citationCount":"0","resultStr":"{\"title\":\"Risk prediction of acute variceal bleeding in hepatocellular carcinoma patients undergoing systemic therapy based on immune checkpoint inhibitors.\",\"authors\":\"Xu Zhang, Li-Meng Song, Yu-Piao Zheng, Bao-Xin Qian, Jing Liang, Feng-Mei Wang\",\"doi\":\"10.4251/wjgo.v17.i8.108887\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Acute variceal bleeding (AVB) represents a life-threatening complication in hepatocellular carcinoma (HCC) patients undergoing systemic therapy, mainly including immune checkpoint inhibitors (ICIs) and antivascular drugs used alone or in combination. The pathogenesis of AVB in this population may involve tumor-related factors, treatment-induced effects, or progression of underlying portal hypertension. Identifying high-risk factors for AVB is crucial for the management of this patient population.</p><p><strong>Aim: </strong>To develop and validate a risk prediction model for AVB occurrence in cirrhotic HCC patients receiving ICI-based systemic therapy.</p><p><strong>Methods: </strong>This retrospective study analyzed 286 HCC patients (2021-2022) receiving ICIs (mono-/combination therapy), randomly split into training (<i>n</i> = 184) and validation (<i>n</i> = 102) cohorts. In the training cohort, bleeding <i>vs</i> non-bleeding groups were compared for general information, etiological data, laboratory indicators, tumor staging, systemic treatment drugs, variceal bleeding history, and endoscopic treatment history. Risk factors for AVB were identified and used to establish a logistic regression model for predicting bleeding, which was further validated in the validation cohort.</p><p><strong>Results: </strong>The bleeding group had significantly higher proportions of patients with platelet count ≥ 100 × 10<sup>9</sup>/L, alpha-fetoprotein ≥ 400 ng/mL, tumor diameter ≥ 5 cm, portal vein tumor thrombosis, ascites, bleeding history, prior endoscopic treatment, albumin-bilirubin grade level 2-3, fibrosis-4 index (FIB-4) ≥ 4.57, and prognostic nutritional index < 45 compared to the non-bleeding group. Multivariate analysis identified tumor diameter ≥ 5 cm, portal vein thrombosis, bleeding history, and elevated FIB-4 as independent risk factors for bleeding (<i>P</i> < 0.05). A predictive model based on these factors showed good discrimination, with area under the receiver operating characteristic curve values of 0.861 (training) and 0.816 (validation).</p><p><strong>Conclusion: </strong>A history of pre-ICI bleeding significantly increases recurrent bleeding risk, necessitating close monitoring. The FIB-4 fibrosis model, combined with tumor features, can also serve as a predictive factor for bleeding.</p>\",\"PeriodicalId\":23762,\"journal\":{\"name\":\"World Journal of Gastrointestinal Oncology\",\"volume\":\"17 8\",\"pages\":\"108887\"},\"PeriodicalIF\":2.5000,\"publicationDate\":\"2025-08-15\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12362552/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"World Journal of Gastrointestinal Oncology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4251/wjgo.v17.i8.108887\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"World Journal of Gastrointestinal Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4251/wjgo.v17.i8.108887","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Risk prediction of acute variceal bleeding in hepatocellular carcinoma patients undergoing systemic therapy based on immune checkpoint inhibitors.
Background: Acute variceal bleeding (AVB) represents a life-threatening complication in hepatocellular carcinoma (HCC) patients undergoing systemic therapy, mainly including immune checkpoint inhibitors (ICIs) and antivascular drugs used alone or in combination. The pathogenesis of AVB in this population may involve tumor-related factors, treatment-induced effects, or progression of underlying portal hypertension. Identifying high-risk factors for AVB is crucial for the management of this patient population.
Aim: To develop and validate a risk prediction model for AVB occurrence in cirrhotic HCC patients receiving ICI-based systemic therapy.
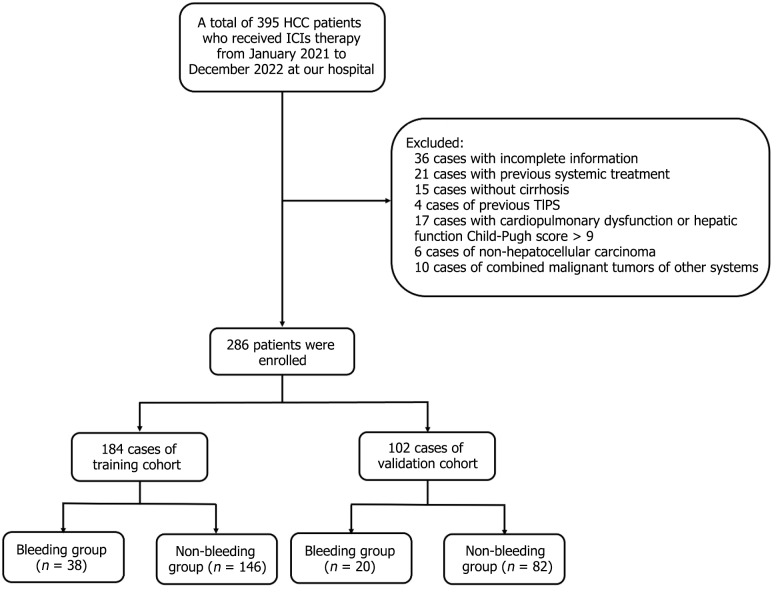
Methods: This retrospective study analyzed 286 HCC patients (2021-2022) receiving ICIs (mono-/combination therapy), randomly split into training (n = 184) and validation (n = 102) cohorts. In the training cohort, bleeding vs non-bleeding groups were compared for general information, etiological data, laboratory indicators, tumor staging, systemic treatment drugs, variceal bleeding history, and endoscopic treatment history. Risk factors for AVB were identified and used to establish a logistic regression model for predicting bleeding, which was further validated in the validation cohort.
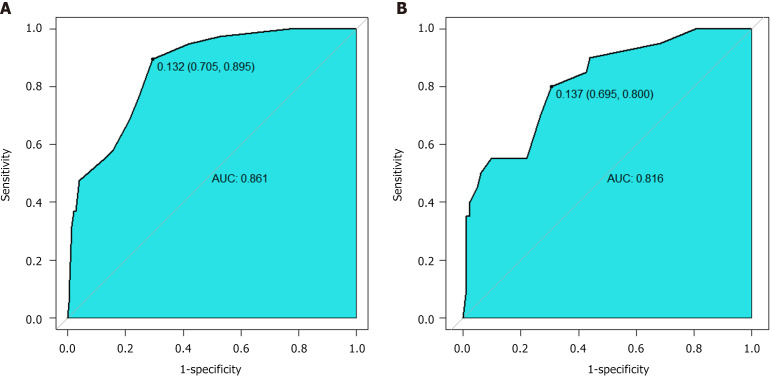
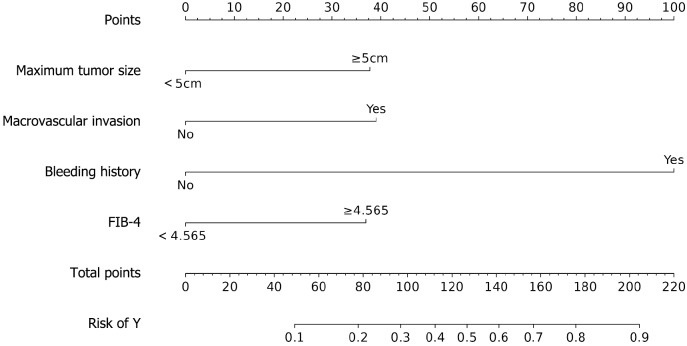
Results: The bleeding group had significantly higher proportions of patients with platelet count ≥ 100 × 109/L, alpha-fetoprotein ≥ 400 ng/mL, tumor diameter ≥ 5 cm, portal vein tumor thrombosis, ascites, bleeding history, prior endoscopic treatment, albumin-bilirubin grade level 2-3, fibrosis-4 index (FIB-4) ≥ 4.57, and prognostic nutritional index < 45 compared to the non-bleeding group. Multivariate analysis identified tumor diameter ≥ 5 cm, portal vein thrombosis, bleeding history, and elevated FIB-4 as independent risk factors for bleeding (P < 0.05). A predictive model based on these factors showed good discrimination, with area under the receiver operating characteristic curve values of 0.861 (training) and 0.816 (validation).
Conclusion: A history of pre-ICI bleeding significantly increases recurrent bleeding risk, necessitating close monitoring. The FIB-4 fibrosis model, combined with tumor features, can also serve as a predictive factor for bleeding.
期刊介绍:
The World Journal of Gastrointestinal Oncology (WJGO) is a leading academic journal devoted to reporting the latest, cutting-edge research progress and findings of basic research and clinical practice in the field of gastrointestinal oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


